

Two-stage pancreatic head resection after previous damage control surgery in trauma: two rare case reports
- PMID: 32397989
- PMCID: PMC7216496
- DOI: 10.1186/s12893-020-00763-2
Two-stage pancreatic head resection after previous damage control surgery in trauma: two rare case reports
Abstract
Background: This study describes the successful treatment of two clinical settings of grade V pancreaticoduodenal blunt trauma only possible due to the prompt collaboration of a peripheral trauma hospital and a central hepatobiliary and pancreatic unit.
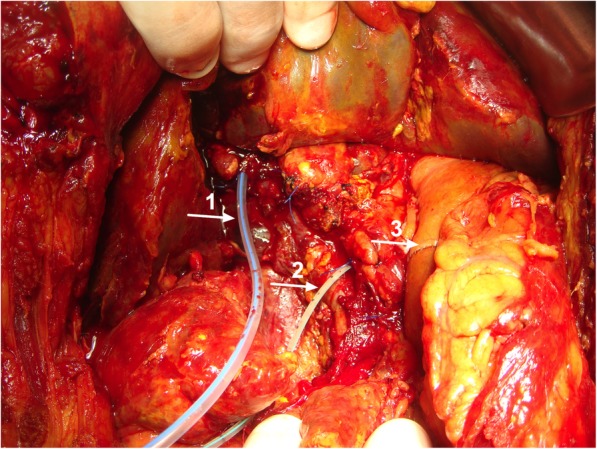
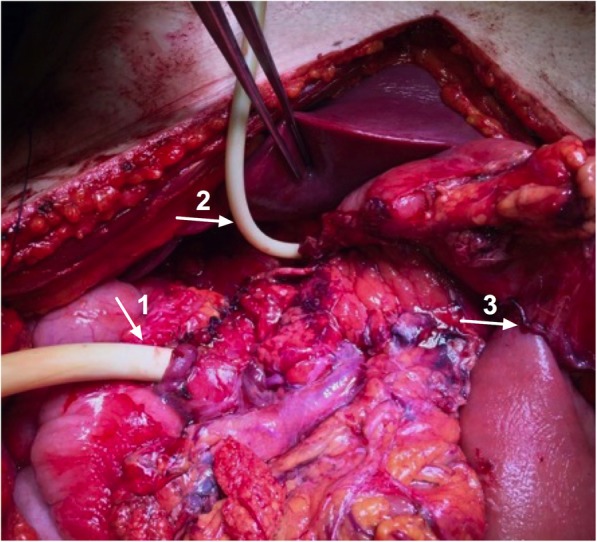
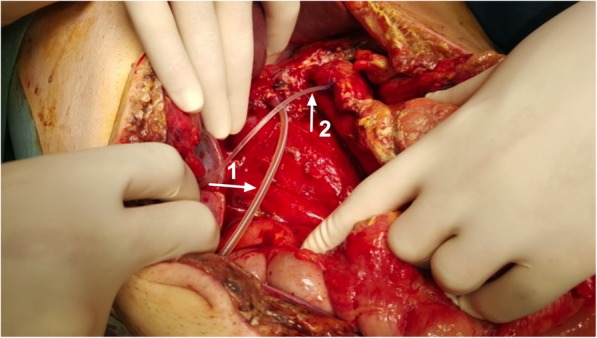
Case presentation: We reviewed the clinical records of two male patients aged 17 and 47 years old who underwent a two-stage pancreaticoduodenectomy after a previous Damage-Control Surgery (DCS). Both patients were transferred to our Hepatobiliopancreatic Unit 2 days after immediate DCS with haemostasis, debridement, duodenostomy, gastroenterostomy, external drainage and laparostomy. One day after, they both underwent a two-stage Whipple's procedure with external cannulation of the main bile duct and the main pancreatic duct with seized calibre silicone drains through the skin. The reconstructive phase was performed two weeks later. The first patient had an uneventful post-operative course and was discharged on post-operative day 8. The second patient developed a high debt biliary fistula on post-operative day 5 being submitted to a relaparotomy with extensive peritoneal lavage. After conservative measures the fistula underwent a progressive closure in 15 days, and the patient was discharged at post-operative day 50 without any limitations.
Conclusions: Pancreaticoduodenectomy is a life-saving operation in selected grade V pancreaticoduodenal trauma lesions. DCS is a salvage approach, often performed in peripheral hospitals, making an early referral to an hepatobiliopancreatic centre mandatory to achieve survival in these severely injured patients. A two-staged Whipple's operation for severe duodenal / pancreatic trauma can be performed safely and may represent a life-saving option under these very unusual circumstances.
Keywords: Case reports; Duodenal trauma; Pancreatic injury; Pancreatic trauma; Pancreaticoduodenectomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Potoka DA, Gaines BA, Leppaniemi A, Peitzman AB. Management of blunt pancreatic trauma: what's new? Eur J Trauma Emerg Surg. 2015;41(3):239–250. - PubMed
-
- Kollar D, Molnar FT, Zsoldos P, Benedek-Tóth Z, Olah A. Diagnosis and management of blunt pancreatic trauma. Surg Gastroenterol Oncol. 2018;23(1):5–15.
-
- Berne CJ, Donovan AJ, Hagen WE. Combined duodenal pancreatc trauma. The role of end-to-side gastrojejunostomy. Arch Surg. 1968;96(5):712–722. - PubMed
-
- Gagne S, O Sullivan-Murphy B, Lo HS, McIntosh LJ. Pancreaticobiliary trauma: a multimodality imaging update. Semin Ultrasound CT MR. 2018;39(4):355-62. 10.1053/j.sult.2018.03.004. - PubMed
-
- Krige JEJ, Kotze UK, Setshedi M, Nicol AJ, Navsaria PH. Management of pancreatic injuries during damage control surgery: an observational outcomes analysis of 79 patients treated at an academic level 1 trauma Centre. Eur J Trauma Emerg Surg. 2017;43(3):411–420. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
