

The Brazilian Portuguese version of the Exercise Adherence Rating Scale (EARS-Br) showed acceptable reliability, validity and responsiveness in chronic low back pain
- PMID: 32398068
- PMCID: PMC7218635
- DOI: 10.1186/s12891-020-03308-z
The Brazilian Portuguese version of the Exercise Adherence Rating Scale (EARS-Br) showed acceptable reliability, validity and responsiveness in chronic low back pain
Abstract
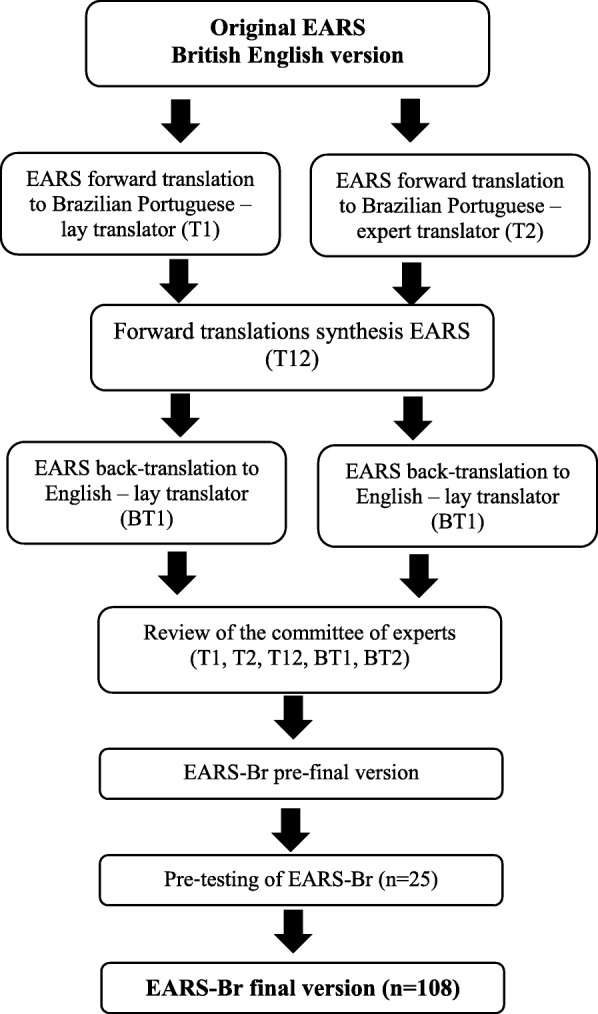
Background: This study aimed to adapt the Exercise Adherence Rating Scale (EARS) into Brazilian Portuguese and evaluate its measurement properties, given as reliability, validity, and responsiveness in patients with non-specific Chronic Low Back Pain (CLBP).
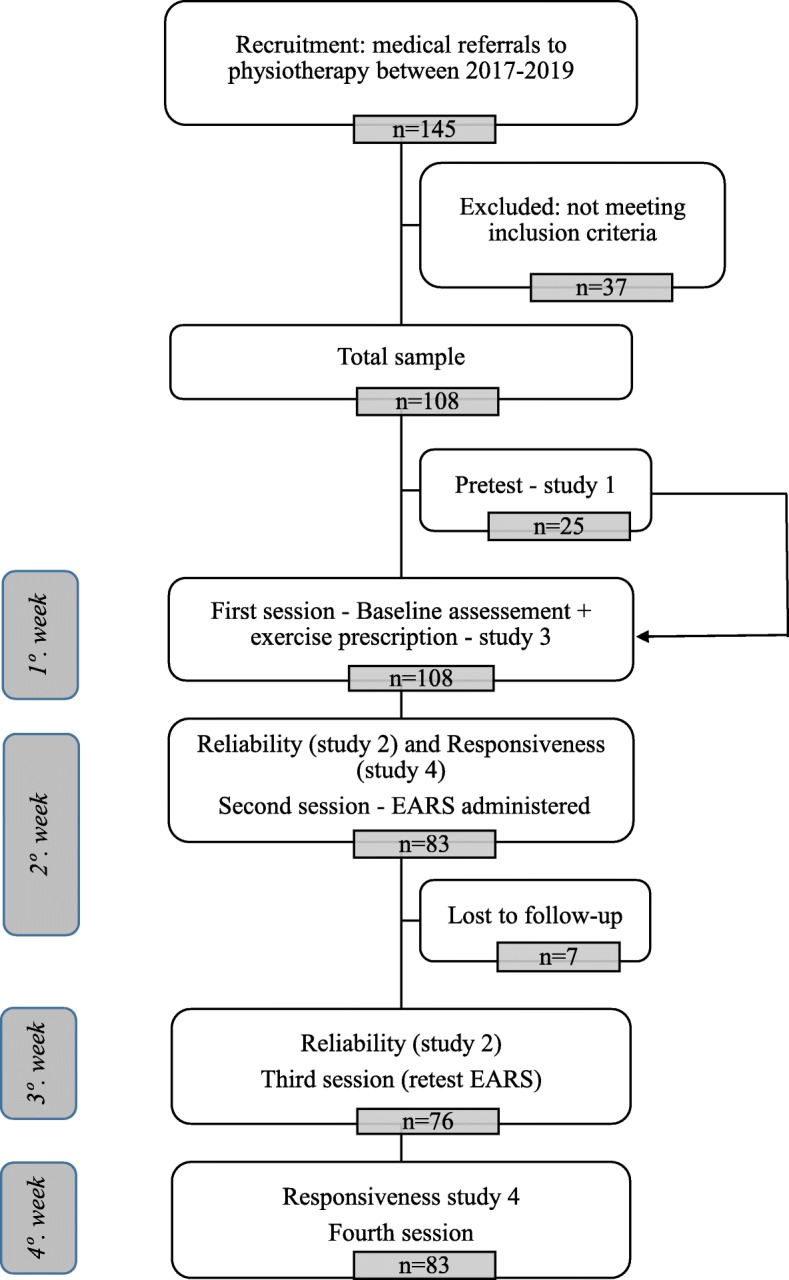
Methods: A total of 108 patients with a mean age of 46.62 years (SD = 9.98) and CLBP participated in this longitudinal study. Participants were oriented on undertaking the prescribed exercises in the first session, and adherence behavior was assessed after 1 week, and finally reassessed after 2 weeks (test-retest reliability). Three weeks after the first assessment, they were invited again to full fill the EARS (responsiveness). The intraclass correlation coefficient (ICC2,1) and Cronbach's α were used to assess test-retest reliability and internal consistency, respectively. Spearman's correlation and confirmatory factor analysis (CFA) were used to assess construct validity, and the Receiver operating characteristic curve and area under the curve (AUC) were used to analyze responsiveness.
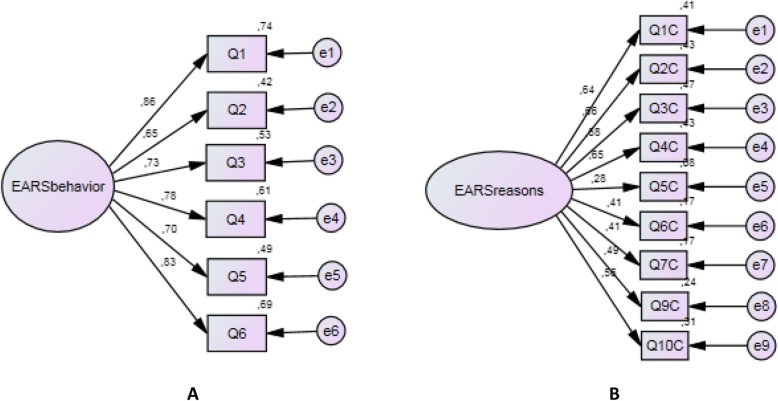
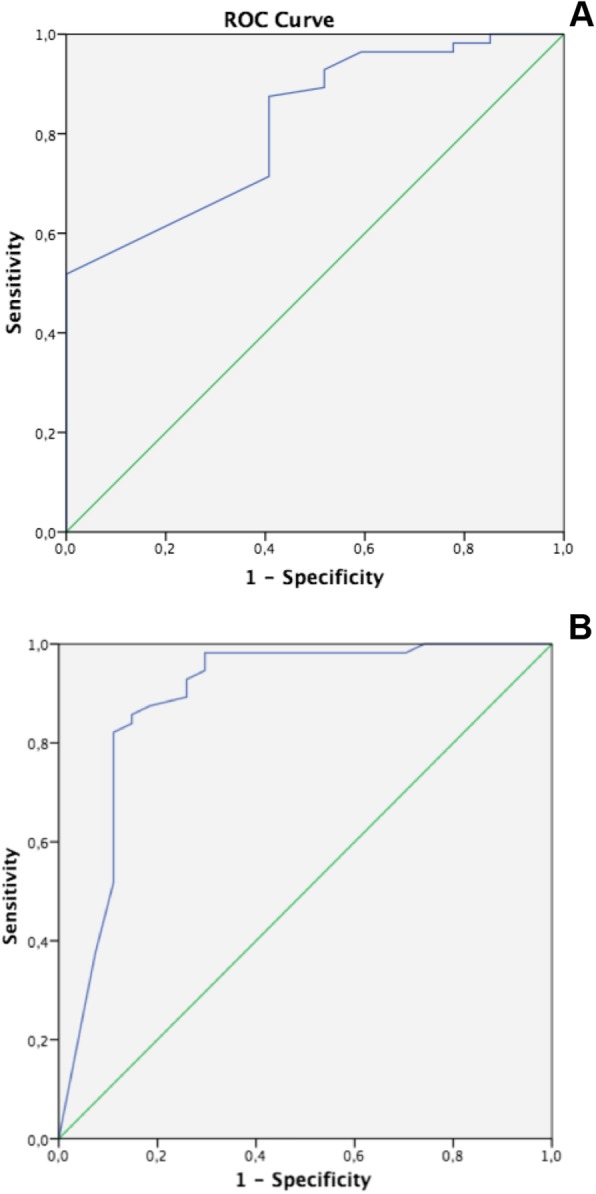
Results: The one-factor EARS-Br (adherence behavior) structure with 6 items showed acceptable fit indexes (comparative fit index and goodness of fit index> 0.90 and root-mean-square error of approximation< 0.08). The EARS-Br scale showed acceptable internal consistency (α = 0.88) and excellent reliability (ICC = 0.91 [95% CI 0.86-0.94]). Mild to moderate correlations were observed between EARS-Br total score vs. disability, pain catastrophizing, depression/anxiety, fear-avoidance and pain intensity. A Minimally Important Change (MIC) of 5.5 in the EARS-Br total score was considered as a meaningful change in the adherence behavior (AUC = 0.82). Moderate accuracy (AUC = 0.89) was obtained for a 17/24 total EARS cutoff score after home exercise was prescribed. The sensitivity and specificity were also acceptable (greater than 80%).
Conclusion: Our results demonstrated acceptable EARS-Br reliability, validity, and responsiveness for patients with CLBP. A final score of 17/24 on EARS after the prescription of home-exercise could be used as a cut-off for an acceptable adherence behavior associated with improvement in patient outcomes.
Keywords: Adherence; Chronic low Back pain; Prescribed exercise; Responsiveness; Validity studies.
Conflict of interest statement
Not Applicable.
Figures
References
-
- Frost R, Levati S, McClurg D, Brady M, Williams B. What Adherence Measures Should Be Used in Trials of Home-Based Rehabilitation Interventions? A Systematic Review of the Validity, Reliability, and Acceptability of Measures. Arch Phys Med Rehabil. 2017; 98(6):1241–1256.e45. - PubMed
-
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M; Lancet Low Back Pain Series Working Group. What low back pain is and why we need to pay attention. Lancet. 2018, 9;391(10137):2356–2367. - PubMed
-
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017, 18;389(10070):736–747. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
