

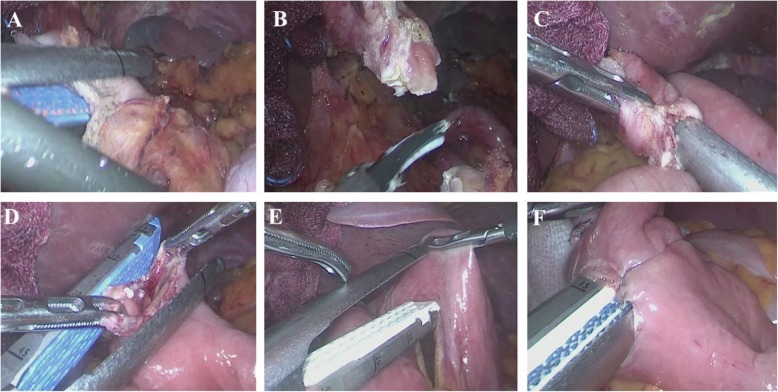
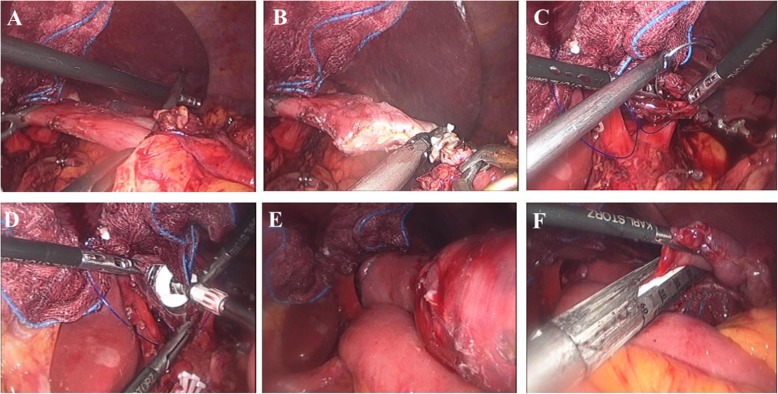
Intracorporeal esophagojejunostomy using a linear stapler in laparoscopic total gastrectomy: comparison with circular stapling technique
- PMID: 32398072
- PMCID: PMC7218545
- DOI: 10.1186/s12893-020-00746-3
Intracorporeal esophagojejunostomy using a linear stapler in laparoscopic total gastrectomy: comparison with circular stapling technique
Abstract
Background: Laparoscopic total gastrectomy for gastric cancer is feasible but less commonly performed compared to laparoscopic distal gastrectomy due to technical difficulties such as reconstruction. There is no standard esophagojejunal anastomosis technique in laparoscopic total gastrectomy due to a lack of evidence.
Methods: We retrospectively analyzed data from 213 patients with gastric cancer who underwent laparoscopic total gastrectomy from October 2012 to December 2016. Of these, 109 and 104 patients underwent esophagojejunostomy with linear and circular stapling, respectively. We compared short-term postoperative outcomes, including surgical complications and anastomosis costs between both groups.
Results: The mean operation time in the linear stapler group was longer than the circular stapler group (Linear stapler, 235.3 ± 57.9 vs. Circular stapler, 217.1 ± 55.8 min; P = 0.021); however, D2 lymph node dissection was performed more in the linear stapler group (Linear stapler, 36.7% vs. Circular stapler, 23.1%; P = 0.030). There were two anastomosis leakages in each group (Linear stapler, 1.8% vs. Circular stapler, 1.9%; P > 0.999). Anastomosis stenosis only occurred in the circular stapler group (Linear stapler, 0% vs. Circular stapler, 7.7%; P = 0.003). Although the linear stapling technique used more stapler cartridges (Linear stapler, 7.6 ± 1.1 vs. Circular stapler, 4.8 ± 0.9; P < 0.001), costs related to anastomosis were lower in the linear stapler group (Linear stapler, 1,904,679 ± 342,116 vs. Circular stapler, 2,246,150 ± 427,136KRW; P < 0.001).
Conclusions: Esophagojejunostomy with the linear stapling technique reduces anastomosis stenosis in laparoscopic total gastrectomy. It can be recommended as a safe and more cost-effective method for esophagojejunal anastomosis.
Keywords: Circular stapler; Esophagojejunostomy; Laparoscopic total gastrectomy; Linear stapler; Stenosis.
Conflict of interest statement
Dr. Woo Jin Hyung has stock in Hutom, received research grants from Medtronic and GC Pharma, and is a consultant for Ethicon and Verb Surgical. Sejin Lee, Harim Lee, Jeong Ho Song, Seohee Choi, Minah Cho, Taeil Son, and Hyoung-Il Kim have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Kim W, Kim HH, Han SU, Kim MC, Hyung WJ, Ryu SW, et al. Decreased morbidity of laparoscopic distal gastrectomy compared with open distal Gastrectomy for stage I gastric cancer: short-term outcomes from a multicenter randomized controlled trial (KLASS-01) Ann Surg. 2016;263(1):28–35. doi: 10.1097/SLA.0000000000001346. - DOI - PubMed
-
- Katai H, Mizusawa J, Katayama H, Takagi M, Yoshikawa T, Fukagawa T, et al. Short-term surgical outcomes from a phase III study of laparoscopy-assisted versus open distal gastrectomy with nodal dissection for clinical stage IA/IB gastric cancer: Japan clinical oncology group study JCOG0912. Gastric Cancer. 2017;20(4):699–708. doi: 10.1007/s10120-016-0646-9. - DOI - PubMed
-
- Lee HJ, Hyung WJ, Yang HK, Han SU, Park YK, An JY, et al. Short-term outcomes of a multicenter randomized controlled trial comparing laparoscopic distal Gastrectomy with D2 lymphadenectomy to open distal Gastrectomy for locally advanced gastric cancer (KLASS-02-RCT). Ann Surg. 2019. 10.1097/SLA.0000000000003217. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
