

Bacteremia Antibiotic Length Actually Needed for Clinical Effectiveness (BALANCE) randomised clinical trial: study protocol
- PMID: 32398341
- PMCID: PMC7223357
- DOI: 10.1136/bmjopen-2020-038300
Bacteremia Antibiotic Length Actually Needed for Clinical Effectiveness (BALANCE) randomised clinical trial: study protocol
Abstract
Introduction: Bloodstream infections are a leading cause of mortality and morbidity; the duration of treatment for these infections is understudied.
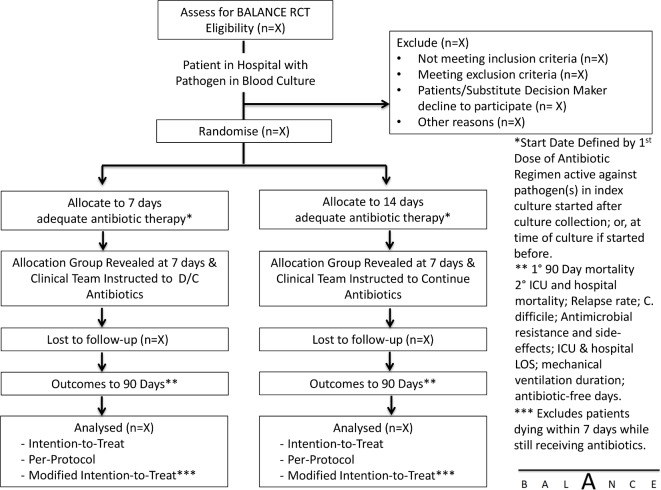
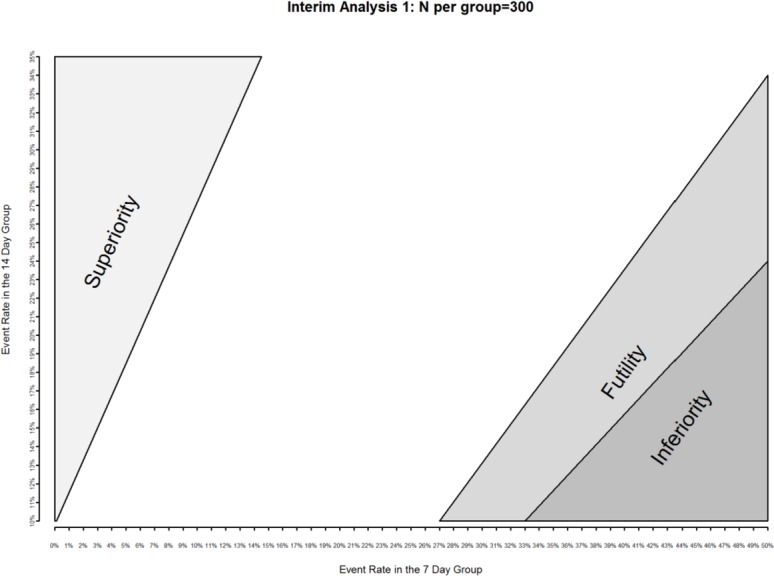
Methods and analysis: We will conduct an international, multicentre randomised clinical trial of shorter (7 days) versus longer (14 days) antibiotic treatment among hospitalised patients with bloodstream infections. The trial will include 3626 patients across 60 hospitals and 6 countries. We will include patients with blood cultures confirming a pathogenic bacterium after hospital admission. Exclusion criteria will include patient factors (severe immunosuppression), infection site factors (endocarditis, osteomyelitis, undrained abscesses, infected prosthetic material) and pathogen factors (Staphylococcus aureus, Staphylococcus lugdunensis, Candida and contaminant organisms). We will leave the selection of specific antibiotics, doses and route of delivery to the discretion of treating physicians; no placebo control will be used given the diversity of pathogens and sources of bacteraemia. The intervention will be assignment of treatment duration to be 7 versus 14 days. We will minimise selection bias via central randomisation with variable block sizes, with concealed allocation until day 7 of adequate antibiotic treatment. The primary outcome is 90-day survival; we will test whether 7 days is non-inferior to 14 days of treatment, with a non-inferiority margin of 4% absolute mortality. Secondary outcomes include hospital and intensive care unit (ICU) mortality, relapse rates of bacteraemia, hospital and ICU length of stay, mechanical ventilation and vasopressor duration, antibiotic-free days, Clostridium difficile infection, antibiotic allergy and adverse events and colonisation/infection with antibiotic-resistant organisms.
Ethics and dissemination: The study has been approved by the ethics review board at each participating site. Sunnybrook Health Sciences Centre is the central ethics committee. We will disseminate study results via the Canadian Critical Care Trials Group and other collaborating networks to set the global paradigm for antibiotic treatment duration for non-staphylococcal Gram-positive, Gram-negative and anaerobic bacteraemia, among patients admitted to hospital.
Trial registration number: The BALANCE (Bacteremia Antibiotic Length Actually Needed for Clinical Effectiveness) trial was registered at www.clinicaltrials.gov (registration number: NCT03005145).
Keywords: adult intensive & critical care; bacteriology; infectious diseases.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical