

Right-sided brain lesions predominate among patients with lesional mania: evidence from a systematic review and pooled lesion analysis
- PMID: 32398699
- PMCID: PMC7217919
- DOI: 10.1038/s41398-020-0811-0
Right-sided brain lesions predominate among patients with lesional mania: evidence from a systematic review and pooled lesion analysis
Abstract
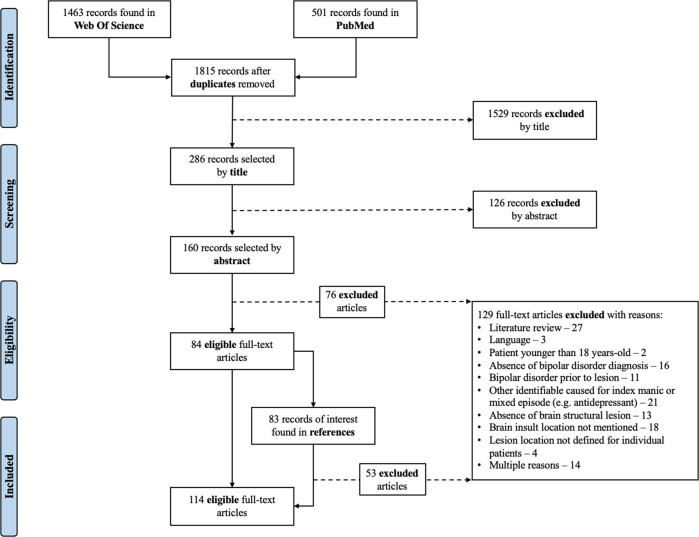
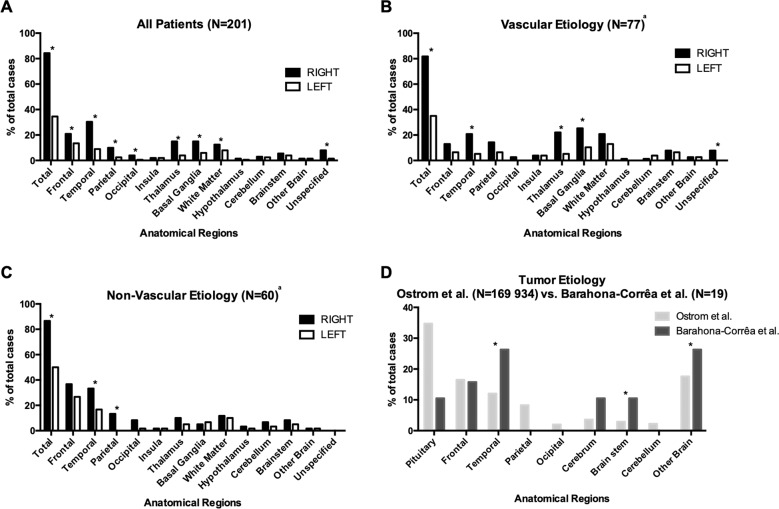
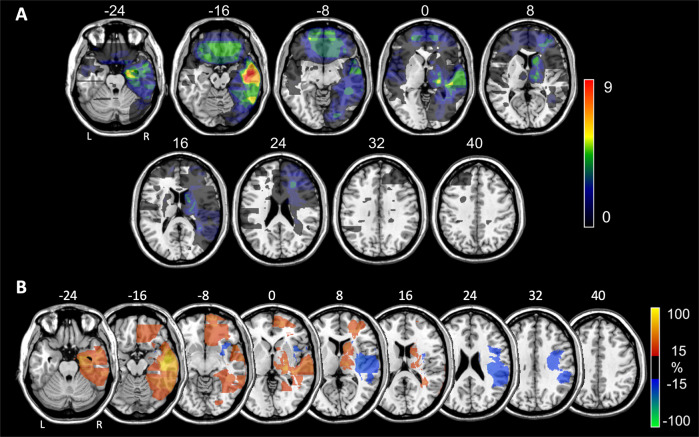
Despite claims that lesional mania is associated with right-hemisphere lesions, supporting evidence is scarce, and association with specific brain areas has not been demonstrated. Here, we aimed to test whether focal brain lesions in lesional mania are more often right- than left-sided, and if lesions converge on areas relevant to mood regulation. We thus performed a systematic literature search (PROSPERO registration CRD42016053675) on PubMed and Web-Of-Science, using terms that reflect diagnoses and structures of interest, as well as lesional mechanisms. Two researchers reviewed the articles separately according to PRISMA Guidelines, selecting reports of adult-onset hypomania, mania or mixed state following a focal brain lesion, for pooled-analyses of individual patient data. Eligible lesion images were manually traced onto the corresponding MNI space slices, and lesion topography analyzed using standard brain atlases. Using this approach, data from 211 lesional mania patients was extracted from 114 reports. Among 201 cases with focal lesions, more patients had lesions involving exclusively the right (60.7%) than exclusively the left (11.4%) hemisphere. In further analyses of 56 eligible lesion images, while findings should be considered cautiously given the potential for selection bias of published lesion images, right-sided predominance of lesions was confirmed across multiple brain regions, including the temporal lobe, fusiform gyrus and thalamus. These, and several frontal lobe areas, were also identified as preferential lesion sites in comparisons with control lesions. Such pooled-analyses, based on the most comprehensive dataset of lesional mania available to date, confirm a preferential association with right-hemisphere lesions, while suggesting that several brain areas/circuits, relevant to mood regulation, are most frequently affected.
Conflict of interest statement
JBB-C received honoraria as member of a local Advisory Board (Trevicta) from Janssen-Cilag, Ltd. GC was supported by Fundação para a Ciência e Tecnologia (FCT) through a PhD Scholarship (SFRH/BD/130210/2017). AJO-M was supported by FCT through a Junior Research and Career Development Award from the Harvard Medical Portugal Program (HMSP/ICJ/0020/2011). JBB-C and AJO-M are supported by grant FCT-PTDC/MEC-PSQ/30302/2017-IC&DT-LISBOA-01-0145-FEDER, funded by national funds from FCT/MCTES and co-funded by FEDER, under the Partnership Agreement Lisboa 2020 - Programa Operacional Regional de Lisboa. GC and AJO-M are supported by grant FCT-PTDC/MED-NEU/31331/2017, funded by FCT/MCTES. AJO-M is recipient of a grant from Schuhfried GmBH for norming and validation of cognitive tests, and is national coordinator for Portugal of a Non-interventional Study (EDMS-ERI-143085581, 4.0) to characterize a Treatment-Resistant Depression Cohort in Europe, sponsored by Janssen-Cilag Ltd. None of the aforementioned agencies had a role in the design and conduct of the study, in the collection, management, analysis, and interpretation of the data, in the preparation, review, or approval of the manuscript, nor in the decision to submit the manuscript for publication. The remaining authors declare that they have no potential conflicts of interest involving this work, including relevant financial activities outside the submitted work and any other relationships or activities that readers could perceive to have influenced, or that give the appearance of potentially influencing what is written.
Figures
References
-
- Stein, G., Wilkinson, G. Seminars in General Adult Psychiatry (RCPsych Publications, 2007).
-
- Krauthammer C, Klerman GL. Secondary mania: manic syndromes associated with antecedent physical illness or drugs. Arch. Gen. Psychiatry. 1978;35:1333–1339. - PubMed
-
- Satzer D, Bond DJ. Mania secondary to focal brain lesions: implications for understanding the functional neuroanatomy of bipolar disorder. Bipolar Disord. 2016;18:205–220. - PubMed
-
- Morken G, Vaaler AE, Folden GE, Andreassen OA, Malt UF. Age at onset of first episode and time to treatment in in-patients with bipolar disorder. Br. J. Psychiatry. 2009;194:559–560. - PubMed
-
- Braun CM, Daigneault R, Gaudelet S, Guimond A. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition symptoms of mania: which one(s) result(s) more often from right than left hemisphere lesions? Compr. Psychiatry. 2008;49:441–459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
