

The impact of surgical simulation on patient outcomes: a systematic review and meta-analysis
- PMID: 32399730
- PMCID: PMC8035110
- DOI: 10.1007/s10143-020-01314-2
The impact of surgical simulation on patient outcomes: a systematic review and meta-analysis
Abstract
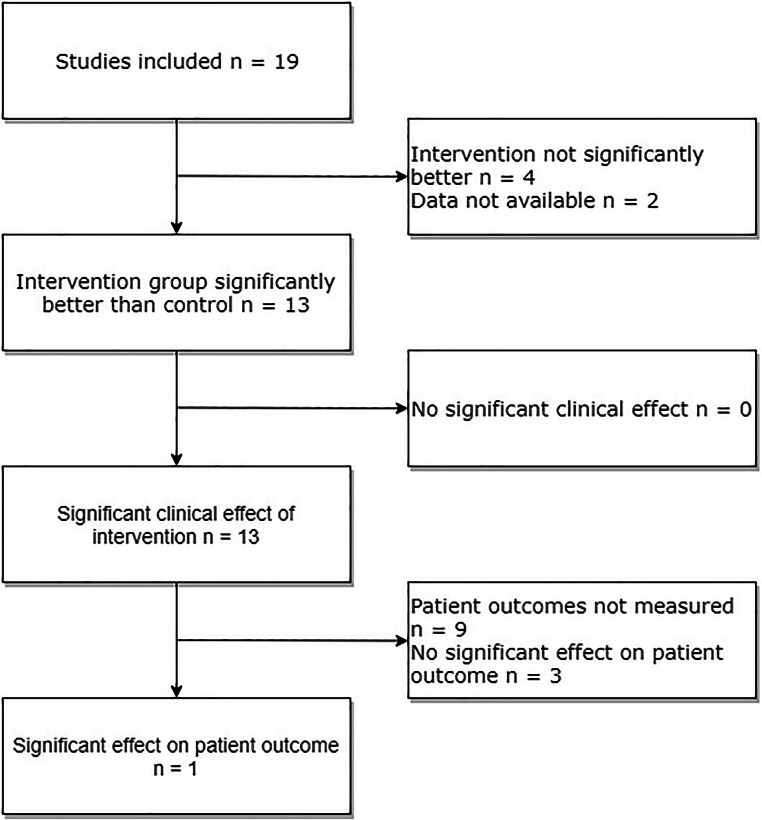
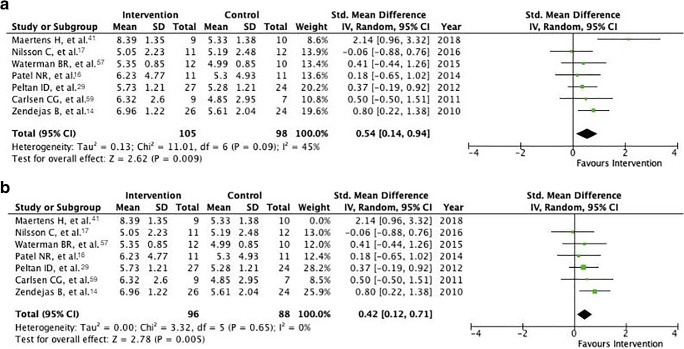
The use of simulation in surgical training is ever growing. Evidence suggests such training may have beneficial clinically relevant effects. The objective of this research is to investigate the effects of surgical simulation training on clinically relevant patient outcomes by evaluating randomized controlled trials (RCT). PubMed was searched using PRISMA guidelines: "surgery" [All Fields] AND "simulation" [All Fields] AND "patient outcome" [All Fields]. Of 119 papers identified, 100 were excluded for various reasons. Meta-analyses were conducted using the inverse-variance random-effects method. Nineteen papers were reviewed using the CASP RCT Checklist. Sixteen studies looked at surgical training, two studies assessed patient-specific simulator practice, and one paper focused on warming-up on a simulator before performing surgery. Median study population size was 22 (range 3-73). Most articles reported outcome measures such as post-intervention Global Rating Scale (GRS) score and/or operative time. On average, the intervention group scored 0.42 (95% confidence interval 0.12 to 0.71, P = 0.005) points higher on a standardized GRS scale of 1-10. On average, the intervention group was 44% (1% to 87%, P = 0.04) faster than the control group. Four papers assessed the impact of simulation training on patient outcomes, with only one finding a significant effect. We found a significant effect of simulation training on operative performance as assessed by GRS, albeit a small one, as well as a significant reduction to operative time. However, there is to date scant evidence from RCTs to suggest a significant effect of surgical simulation training on patient outcomes.
Keywords: Education; Meta-analysis; Neurosurgery; Patient outcome; Simulation; Surgery; Systematic review.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Imber G. Genius on the edge: the bizarre double life of Dr. William Stewart Halsted. New York: Kaplan Pub; 2010.
-
- Ahlberg G, Enochsson L, Gallagher AG, et al. Proficiency-based virtual reality training significantly reduces the error rate for residents during their first 10 laparoscopic cholecystectomies. Am J Surg. 2007;193(6):797–804. - PubMed
-
- Wood D, Wood H. Vygotsky, Tutoring and learning. Oxford Rev Educ. 1996;22(1):5–16.
-
- Kohn LT, Corrigan J, Donaldson MS, Institute of Medicine (U.S.). Committee on Quality of Health Care in America . To err is human: building a safer health system. Washington, D.C.: National Academy Press; 2000. - PubMed
-
- Chief Medical Officer . Good doctors, safer patients: proposals to strengthen the system to assure and improve the performance of doctors and to protect the safety of patients. London: Department of Health, Great Britain; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
