

Circulating Anodic Antigen (CAA): A Highly Sensitive Diagnostic Biomarker to Detect Active Schistosoma Infections-Improvement and Use during SCORE
- PMID: 32400344
- PMCID: PMC7351307
- DOI: 10.4269/ajtmh.19-0819
Circulating Anodic Antigen (CAA): A Highly Sensitive Diagnostic Biomarker to Detect Active Schistosoma Infections-Improvement and Use during SCORE
Abstract
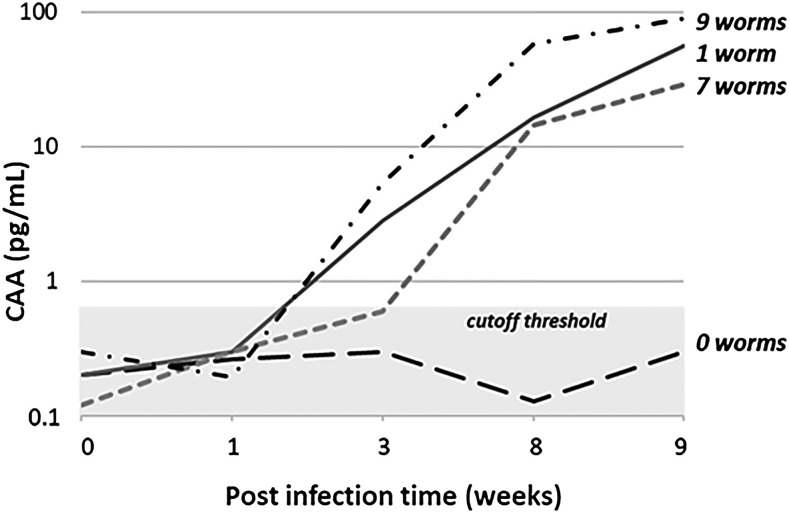
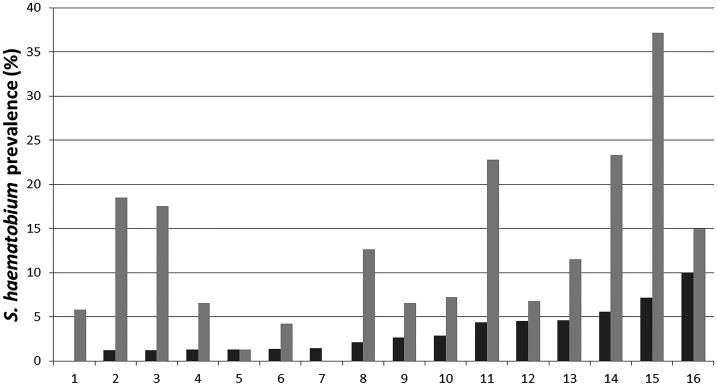
The Schistosomiasis Consortium for Operational Research and Evaluation (SCORE) was funded in 2008 to conduct research that would support country schistosomiasis control programs. As schistosomiasis prevalence decreases in many places and elimination is increasingly within reach, a sensitive and specific test to detect infection with Schistosoma mansoni and Schistosoma haematobium has become a pressing need. After obtaining broad input, SCORE supported Leiden University Medical Center (LUMC) to modify the serum-based antigen assay for use with urine, simplify the assay, and improve its sensitivity. The urine assay eventually contributed to several of the larger SCORE studies. For example, in Zanzibar, we demonstrated that urine filtration, the standard parasite egg detection diagnostic test for S. haematobium, greatly underestimated prevalence in low-prevalence settings. In Burundi and Rwanda, the circulating anodic antigen (CAA) assay provided critical information about the limitations of the stool-based Kato-Katz parasite egg-detection assay for S. mansoni in low-prevalence settings. Other SCORE-supported CAA work demonstrated that frozen, banked urine specimens yielded similar results to fresh ones; pooling of specimens may be a useful, cost-effective approach for surveillance in some settings; and the assay can be performed in local laboratories equipped with adequate centrifuge capacity. These improvements in the assay continue to be of use to researchers around the world. However, additional work will be needed if widespread dissemination of the CAA assay is to occur, for example, by building capacity in places besides LUMC and commercialization of the assay. Here, we review the evolution of the CAA assay format during the SCORE period with emphasis on urine-based applications.
Figures

References
-
- Deelder AM, van Dam GJ, Kornelis D, Fillie YE, van Zeyl RJ, 1996. Schistosoma: analysis of monoclonal antibodies reactive with the circulating antigens CAA and CCA. Parasitology 112: 21–35. - PubMed
-
- Wilson AR, van Dam GJ, Kariuki TM, Farah IO, Deelder AM, Coulson PS, 2006. The detection limits for estimates of infection intensity in schistosomiasis mansoni established by a study in non-human primates. Int J Parasitol 36: 1241–1244. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
