Effect of Internet vs Face-to-Face Cognitive Behavior Therapy for Health Anxiety: A Randomized Noninferiority Clinical Trial
- PMID: 32401286
- PMCID: PMC7221860
- DOI: 10.1001/jamapsychiatry.2020.0940
Effect of Internet vs Face-to-Face Cognitive Behavior Therapy for Health Anxiety: A Randomized Noninferiority Clinical Trial
Abstract
Importance: Health anxiety is a common and often chronic mental health problem associated with distress, substantial costs, and frequent attendance throughout the health care system. Face-to-face cognitive behavior therapy (CBT) is the criterion standard treatment, but access is limited.
Objective: To test the hypothesis that internet-delivered CBT, which requires relatively little resources, is noninferior to face-to-face CBT in the treatment of health anxiety.
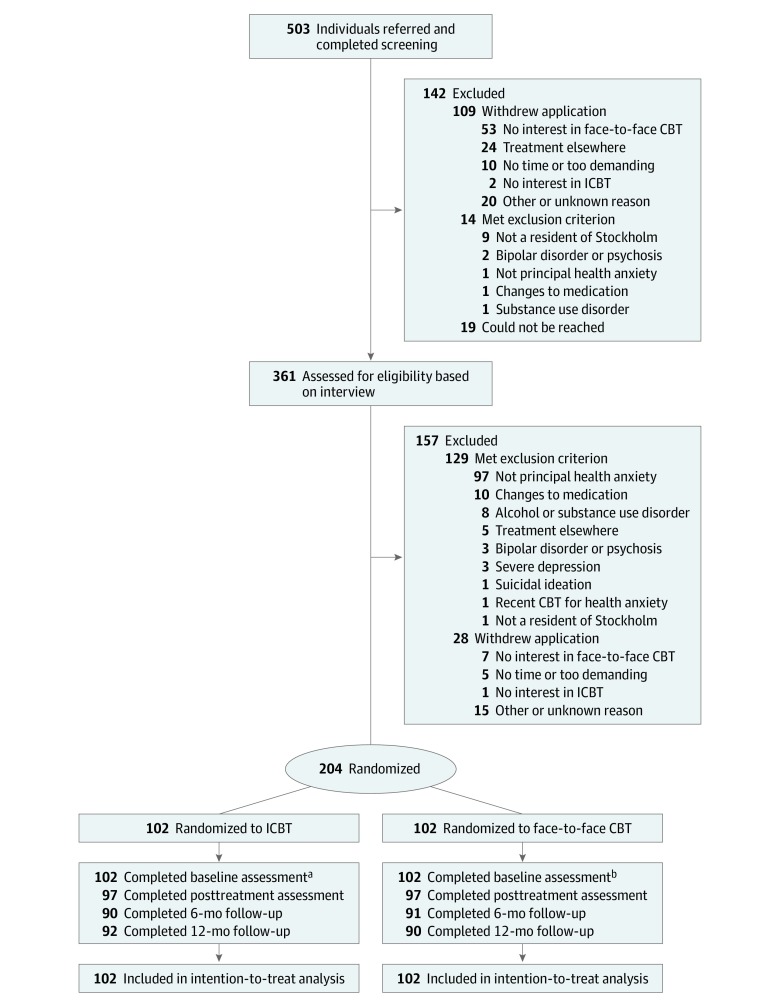
Design, setting, and participants: This randomized noninferiority clinical trial with health economic analysis was based at a primary care clinic and included patients with a principal diagnosis of health anxiety who were self-referred or referred from routine care. Recruitment began in December 10, 2014, and the last treatment ended on July 23, 2017. Follow-up data were collected up to 12 months after treatment. Analysis began October 2017 and ended March 2020.
Interventions: Patients were randomized (1:1) to 12 weeks of internet-delivered CBT or to individual face-to-face CBT.
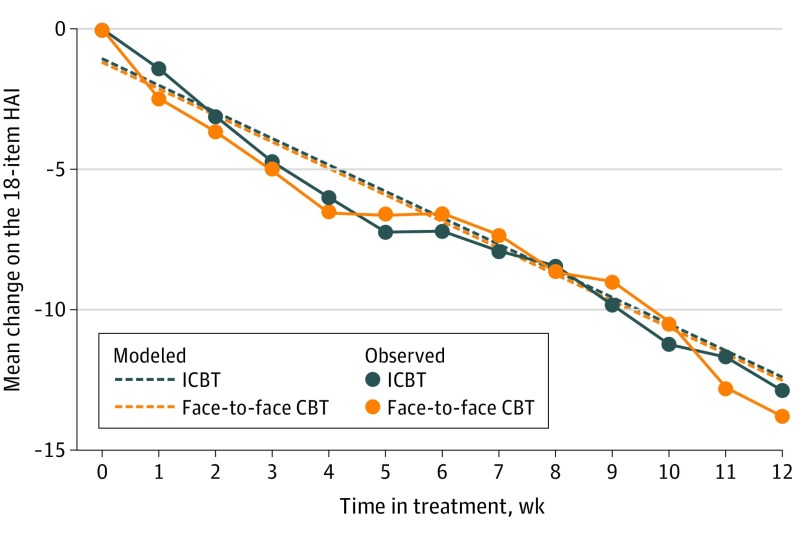
Main outcomes and measures: Change in health anxiety symptoms from baseline to week 12. Analyses were conducted from intention-to-treat and per-protocol (completers only) perspectives, using the noninferiority margin of 2.25 points on the Health Anxiety Inventory, which has a theoretical range of 0 to 54.
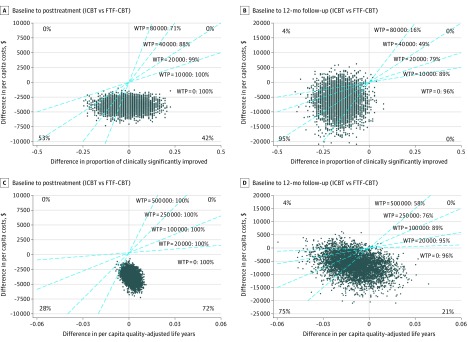
Results: Overall, 204 patients (mean [SD] age, 39 [12] years; 143 women [70%]) contributed with 2386 data points on the Health Anxiety Inventory over the treatment period. Of 204 patients, 102 (50%) were randomized to internet-delivered CBT, and 102 (50%) were randomized to face-to-face CBT. The 1-sided 95% CI upper limits for the internet-delivered CBT vs face-to-face CBT difference in change were within the noninferiority margin in the intention-to-treat analysis (B = 0.00; upper limit: 1.98; Cohen d = 0.00; upper limit: 0.23) and per-protocol analysis (B = 0.01; upper limit: 2.17; Cohen d = 0.00; upper limit: 0.25). The between-group effect was not moderated by initial symptom level, recruitment path, or patient treatment preference. Therapists spent 10.0 minutes per patient per week in the online treatment vs 45.6 minutes for face-to-face CBT. The net societal cost was lower in the online treatment (treatment period point difference: $3854). There was no significant group difference in the number of adverse events, and no serious adverse event was reported.
Conclusions and relevance: In this trial, internet-delivered CBT appeared to be noninferior to face-to-face CBT for health anxiety, while incurring lower net societal costs. The online treatment format has potential to increase access to evidence-based treatment for health anxiety.
Trial registration: ClinicalTrials.gov Identifier: NCT02314065.
Conflict of interest statement
Figures