

Mortality estimates by age and sex among persons living with HIV after ART initiation in Zambia using electronic medical records supplemented with tracing a sample of lost patients: A cohort study
- PMID: 32401797
- PMCID: PMC7219718
- DOI: 10.1371/journal.pmed.1003107
Mortality estimates by age and sex among persons living with HIV after ART initiation in Zambia using electronic medical records supplemented with tracing a sample of lost patients: A cohort study
Abstract
Background: Men in sub-Saharan Africa have lower engagement and retention in HIV services compared to women, which may result in differential survival. However, the true magnitude of difference in HIV-related mortality between men and women receiving antiretroviral therapy (ART) is incompletely characterized.
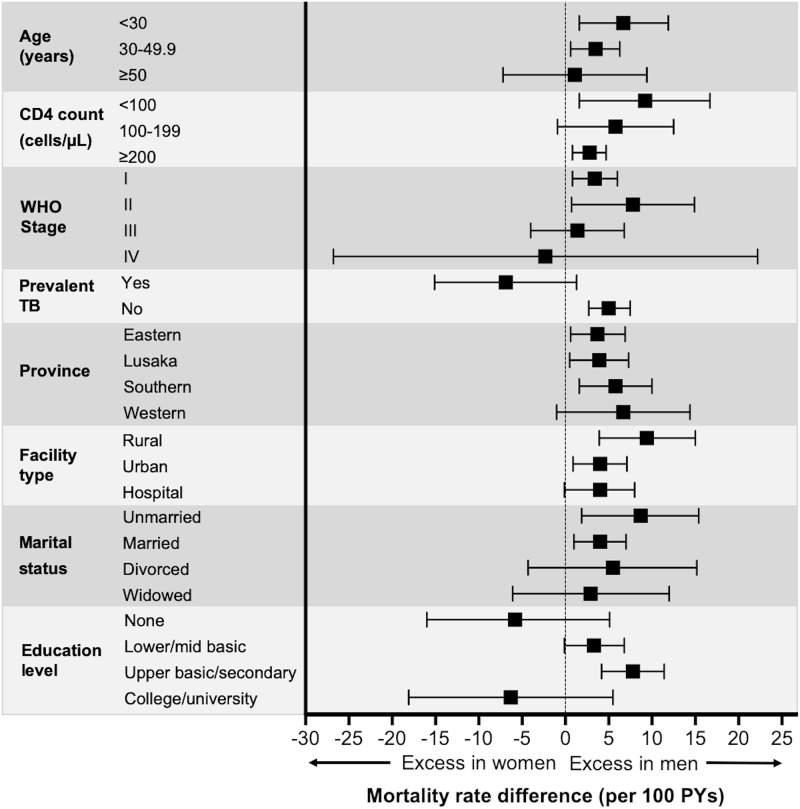
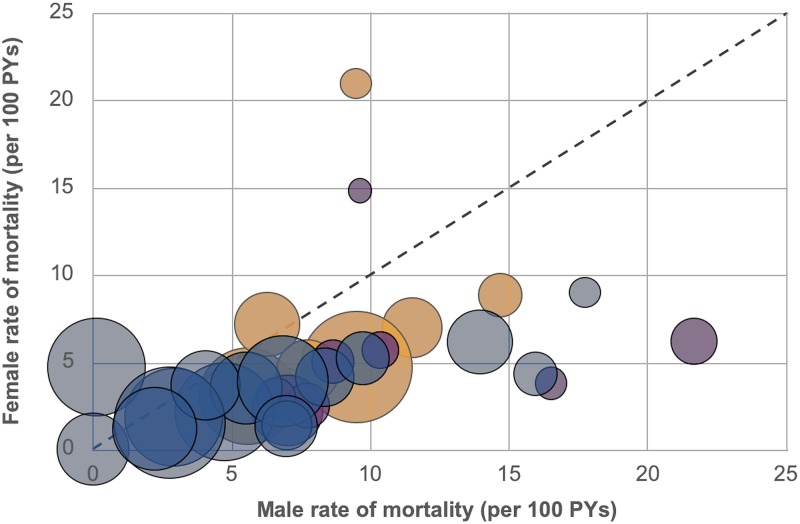
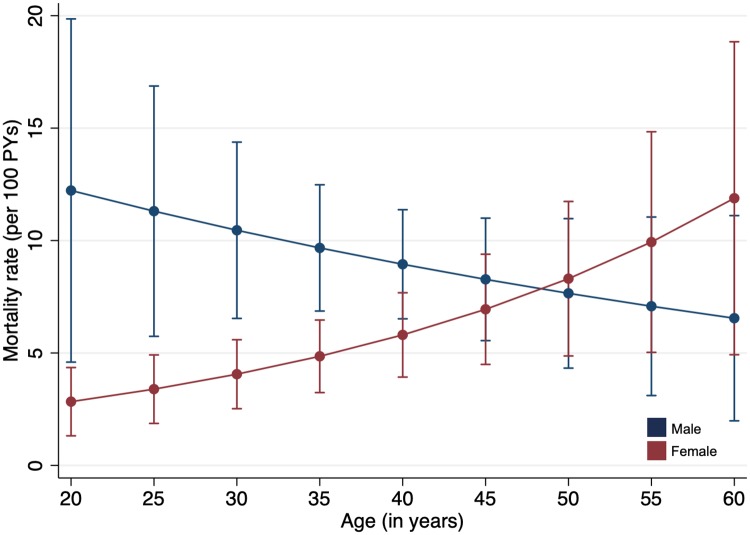
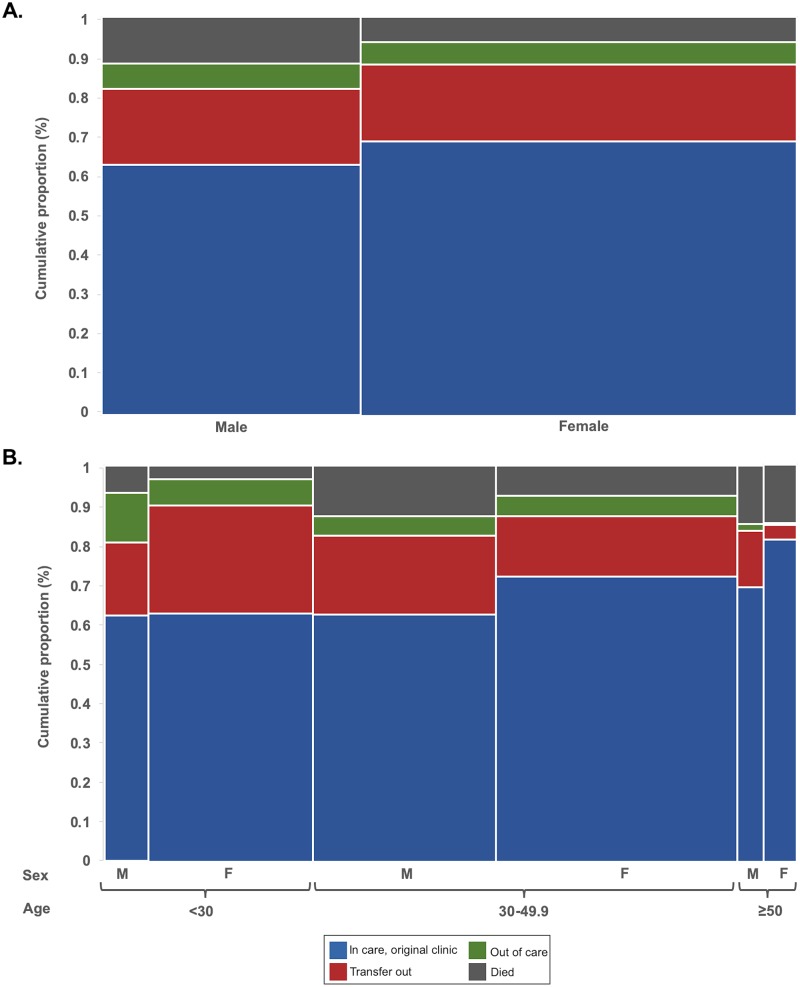
Methods and findings: We evaluated HIV-positive adults ≥18 years old newly initiating ART in 4 Zambian provinces (Eastern, Lusaka, Southern, and Western). In addition to mortality data obtained from routine electronic medical records, we intensively traced a random sample of patients lost to follow-up (LTFU) and incorporated tracing outcomes through inverse probability weights. Sex-specific mortality rates and rate differences were determined using Poisson regression. Parametric g-computation was used to estimate adjusted mortality rates by sex and age. The study included 49,129 adults newly initiated on ART between August 2013 and July 2015; overall, the median age among patients was 35 years, the median baseline CD4 count was 262 cells/μl, and 37.2% were men. Men comprised a smaller proportion of individuals starting ART (37.2% versus 62.8%), tended to be older (median age 37 versus 33 years), and tended to have lower CD4 counts (median 220 versus 289 cells/μl) at the time of ART initiation compared to women. The overall rate of mortality among men was 10.3 (95% CI 8.2-12.4) deaths/100 person-years (PYs), compared to 5.5 (95% CI 4.3-6.8) deaths/100 PYs among women (difference +4.7 [95% CI 2.3-7.2] deaths/100 PYs; p < 0.001). Compared to women in the same age groups, men's mortality rates were particularly elevated among those <30 years old (+6.7 deaths/100 PYs difference), those attending rural health centers (+9.4 deaths/100 PYs difference), those who had an initial CD4 count < 100 cells/μl (+9.2 deaths/100 PYs difference), and those who were unmarried (+8.0 deaths/100 PYs difference). After adjustment for potential confounders and mediators including CD4 count, a substantially higher mortality rate was predicted among men <30 years old compared to women of the same age, while women ≥50 years old had a mortality rate similar to that of age-matched men, but considerably higher than that predicted among young women (<30 years old). No clinically significant differences were evident with respect to rates of facility transfer or care disengagement between men and women. The main study limitations were the inability to successfully ascertain outcomes in all patients selected for tracing and missing clinical and laboratory data due to the use of medical records.
Conclusions: In this study, we found that among HIV-positive adults newly initiating ART, mortality among men exceeded mortality among women; disparities were most pronounced among young patients. Older women, however, also experienced high mortality. Specific interventions for men and older women at highest mortality risk are needed to improve HIV treatment outcomes.
Conflict of interest statement
Elvin Geng is a member of the Editorial Board of PLOS Medicine. All authors otherwise declare no competing interests.
Figures
Similar articles
-
Estimated mortality on HIV treatment among active patients and patients lost to follow-up in 4 provinces of Zambia: Findings from a multistage sampling-based survey.PLoS Med. 2018 Jan 12;15(1):e1002489. doi: 10.1371/journal.pmed.1002489. eCollection 2018 Jan. PLoS Med. 2018. PMID: 29329301 Free PMC article.
-
Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach.PLoS Med. 2019 May 31;16(5):e1002811. doi: 10.1371/journal.pmed.1002811. eCollection 2019 May. PLoS Med. 2019. PMID: 31150380 Free PMC article.
-
Longitudinal engagement trajectories and risk of death among new ART starters in Zambia: A group-based multi-trajectory analysis.PLoS Med. 2019 Oct 29;16(10):e1002959. doi: 10.1371/journal.pmed.1002959. eCollection 2019 Oct. PLoS Med. 2019. PMID: 31661487 Free PMC article.
-
Attrition of HIV-positive children from HIV services in low and middle-income countries.AIDS. 2019 Dec 1;33(15):2375-2386. doi: 10.1097/QAD.0000000000002366. AIDS. 2019. PMID: 31764102 Free PMC article.
-
Strategies to improve antiretroviral therapy (ART) initiation and early engagement among men in sub-Saharan Africa: A scoping review of interventions in the era of universal treatment.Trop Med Int Health. 2023 Jun;28(6):454-465. doi: 10.1111/tmi.13880. Epub 2023 May 2. Trop Med Int Health. 2023. PMID: 37132119 Free PMC article.
Cited by
-
Resistance Testing for Management of HIV Virologic Failure in Sub-Saharan Africa : An Unblinded Randomized Controlled Trial.Ann Intern Med. 2021 Dec;174(12):1683-1692. doi: 10.7326/M21-2229. Epub 2021 Oct 26. Ann Intern Med. 2021. PMID: 34698502 Free PMC article. Clinical Trial.
-
Statistical analysis on the incidence and predictors of death among second-line ART patients in public hospitals of North Wollo and Waghemira Zones, Ethiopia, 2021.Sci Rep. 2024 May 13;14(1):10893. doi: 10.1038/s41598-024-60119-1. Sci Rep. 2024. PMID: 38740783 Free PMC article.
-
Patient-reported Reasons for Stopping Care or Switching Clinics in Zambia: A Multisite, Regionally Representative Estimate Using a Multistage Sampling-based Approach in Zambia.Clin Infect Dis. 2021 Oct 5;73(7):e2294-e2302. doi: 10.1093/cid/ciaa1501. Clin Infect Dis. 2021. PMID: 33011803 Free PMC article.
-
Long-term effect of chronic hepatitis B on mortality in HIV-infected persons in a differential HBV transmission setting.BMC Infect Dis. 2022 May 27;22(1):500. doi: 10.1186/s12879-022-07477-1. BMC Infect Dis. 2022. PMID: 35624437 Free PMC article.
-
Investigating the Determinants of Mortality before CD4 Count Recovery in a Cohort of Patients Initiated on Antiretroviral Therapy in South Africa Using a Fine and Gray Competing Risks Model.Trop Med Infect Dis. 2024 Jul 10;9(7):154. doi: 10.3390/tropicalmed9070154. Trop Med Infect Dis. 2024. PMID: 39058196 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS. Addressing a blind spot in the response to HIV—reaching out to men and boys. Geneva: Joint United Nations Programme on HIV/AIDS; 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
