

Ventricular fibrillation mechanism and global fibrillatory organization are determined by gap junction coupling and fibrosis pattern
- PMID: 32402067
- PMCID: PMC7983010
- DOI: 10.1093/cvr/cvaa141
Ventricular fibrillation mechanism and global fibrillatory organization are determined by gap junction coupling and fibrosis pattern
Abstract
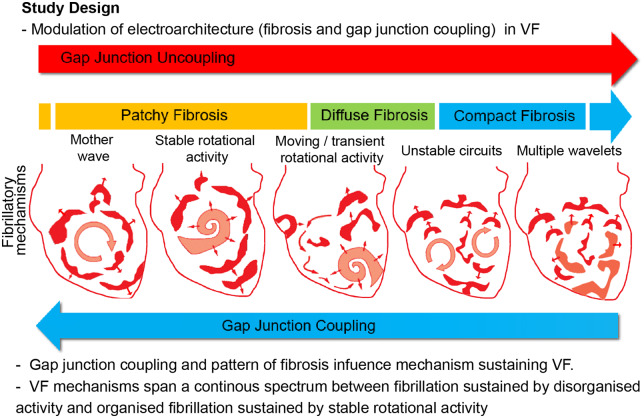
Aims: Conflicting data exist supporting differing mechanisms for sustaining ventricular fibrillation (VF), ranging from disorganized multiple-wavelet activation to organized rotational activities (RAs). Abnormal gap junction (GJ) coupling and fibrosis are important in initiation and maintenance of VF. We investigated whether differing ventricular fibrosis patterns and the degree of GJ coupling affected the underlying VF mechanism.
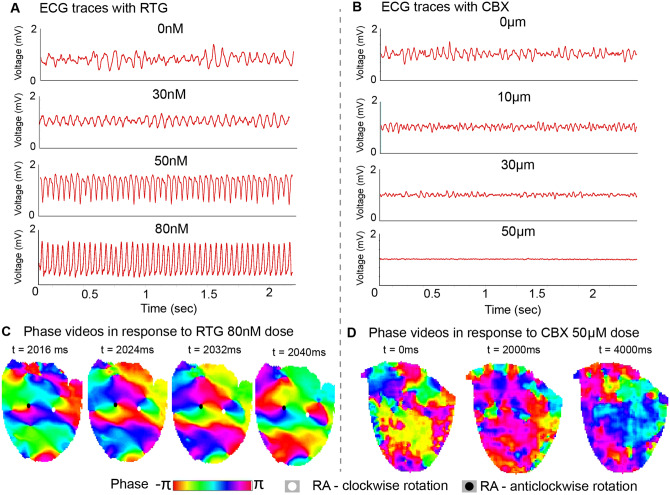
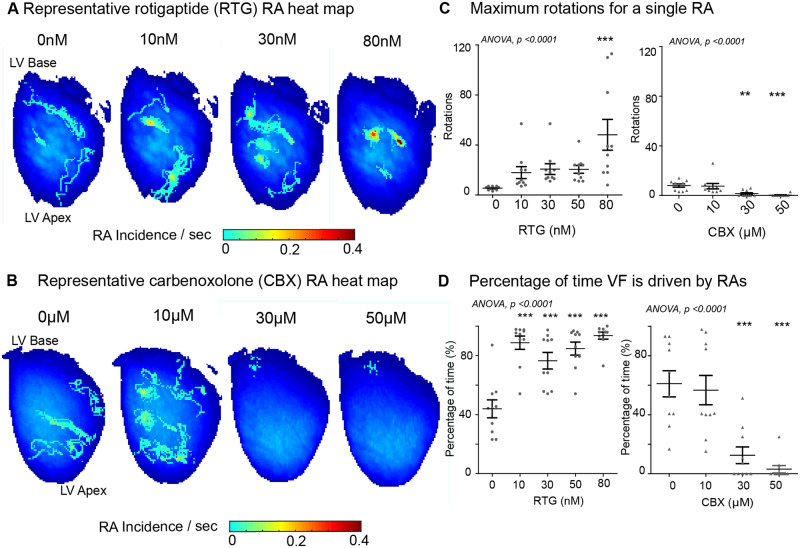
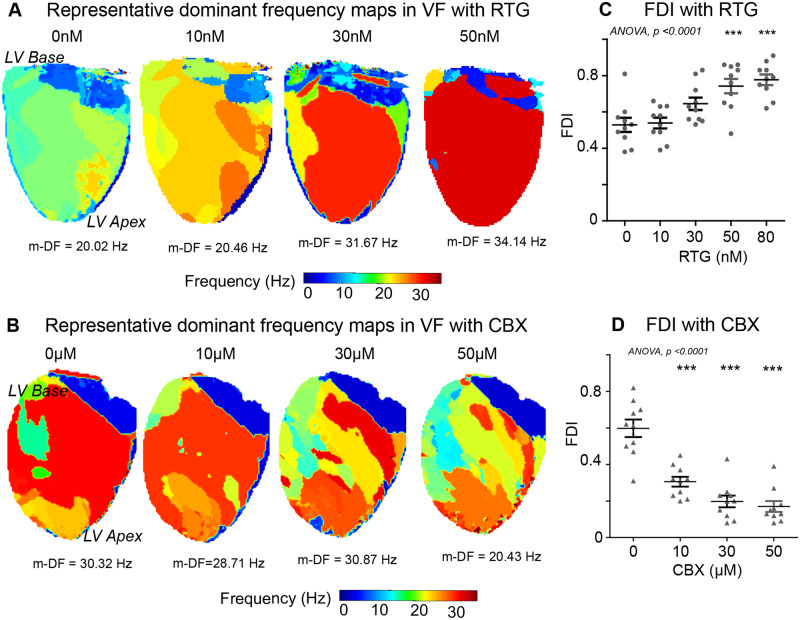
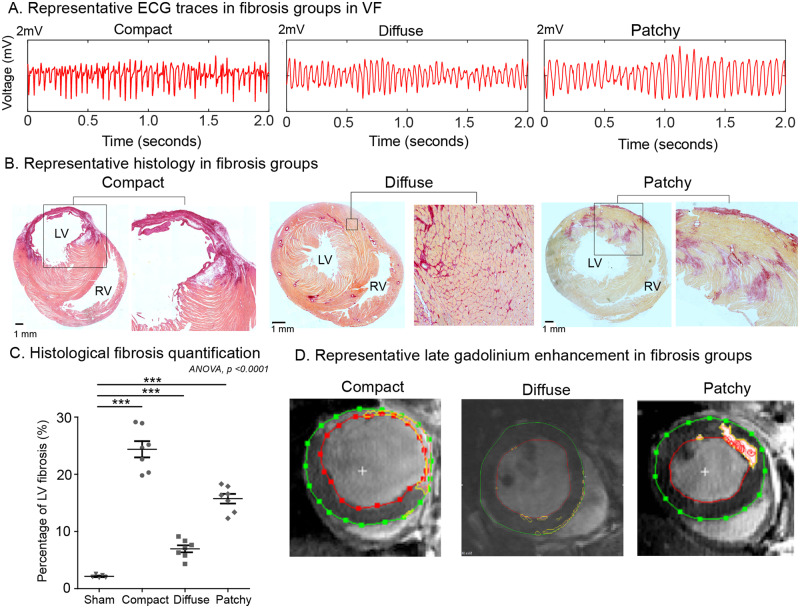
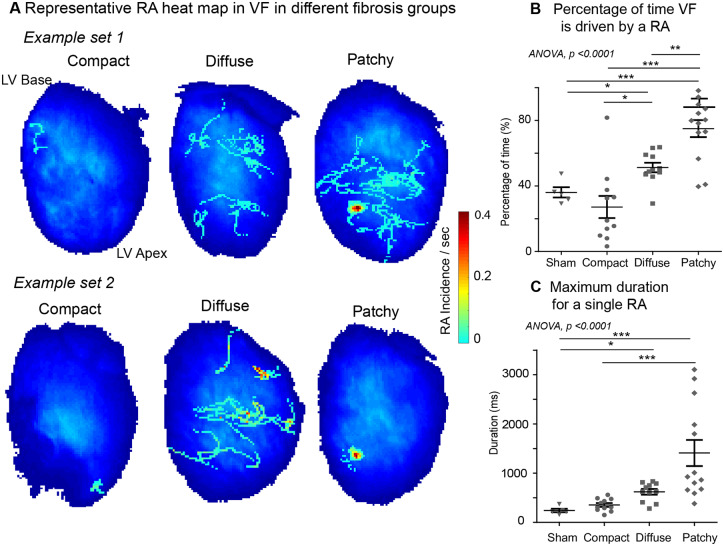
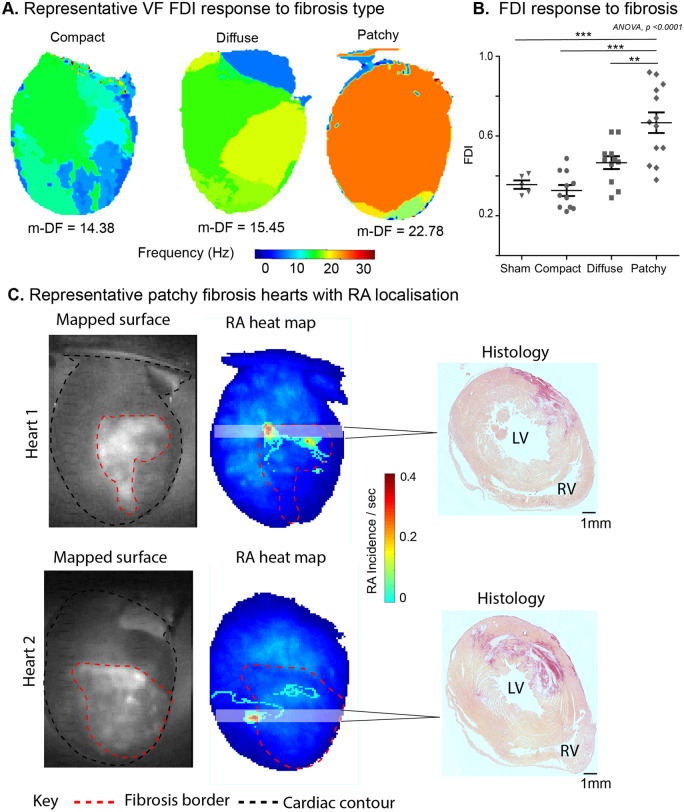
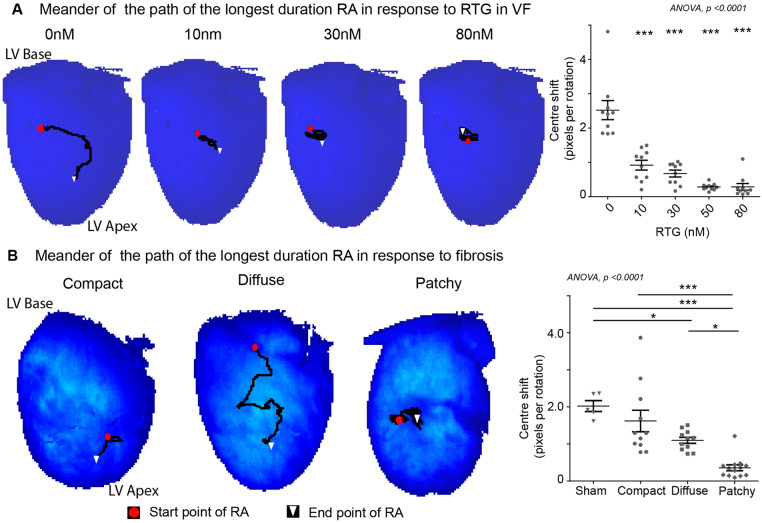
Methods and results: Optical mapping of 65 Langendorff-perfused rat hearts was performed to study VF mechanisms in control hearts with acute GJ modulation, and separately in three differing chronic ventricular fibrosis models; compact fibrosis (CF), diffuse fibrosis (DiF), and patchy fibrosis (PF). VF dynamics were quantified with phase mapping and frequency dominance index (FDI) analysis, a power ratio of the highest amplitude dominant frequency in the cardiac frequency spectrum. Enhanced GJ coupling with rotigaptide (n = 10) progressively organized fibrillation in a concentration-dependent manner; increasing FDI (0 nM: 0.53 ± 0.04, 80 nM: 0.78 ± 0.03, P < 0.001), increasing RA-sustained VF time (0 nM: 44 ± 6%, 80 nM: 94 ± 2%, P < 0.001), and stabilized RAs (maximum rotations for an RA; 0 nM: 5.4 ± 0.5, 80 nM: 48.2 ± 12.3, P < 0.001). GJ uncoupling with carbenoxolone progressively disorganized VF; the FDI decreased (0 µM: 0.60 ± 0.05, 50 µM: 0.17 ± 0.03, P < 0.001) and RA-sustained VF time decreased (0 µM: 61 ± 9%, 50 µM: 3 ± 2%, P < 0.001). In CF, VF activity was disorganized and the RA-sustained VF time was the lowest (CF: 27 ± 7% vs. PF: 75 ± 5%, P < 0.001). Global fibrillatory organization measured by FDI was highest in PF (PF: 0.67 ± 0.05 vs. CF: 0.33 ± 0.03, P < 0.001). PF harboured the longest duration and most spatially stable RAs (patchy: 1411 ± 266 ms vs. compact: 354 ± 38 ms, P < 0.001). DiF (n = 11) exhibited an intermediately organized VF pattern, sustained by a combination of multiple-wavelets and short-lived RAs.
Conclusion: The degree of GJ coupling and pattern of fibrosis influences the mechanism sustaining VF. There is a continuous spectrum of organization in VF, ranging between globally organized fibrillation sustained by stable RAs and disorganized, possibly multiple-wavelet driven fibrillation with no RAs.
Keywords: Fibrillation; Fibrosis; Gap junctions; Mechanisms; Rotational activity; Ventricular fibrillation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Two sides of the same coin: new insights into mechanisms of ventricular fibrillation.Cardiovasc Res. 2021 Mar 21;117(4):983-984. doi: 10.1093/cvr/cvaa246. Cardiovasc Res. 2021. PMID: 33155033 Free PMC article. No abstract available.
References
-
- Nash MP, Mourad A, Clayton RH, Sutton PM, Bradley CP, Hayward M, Paterson DJ, Taggart P.. Evidence for multiple mechanisms in human ventricular fibrillation. Circulation 2006;114:536–542. - PubMed
-
- Nair K, Umapathy K, Farid T, Masse S, Mueller E, Sivanandan RV, Poku K, Rao V, Nair V, Butany J, Ideker RE, Nanthakumar K.. Intramural activation during early human ventricular fibrillation. Circ Arrhythm Electrophysiol 2011;4:692–703. - PubMed
-
- Haïssaguerre M, Hocini M, Cheniti G, Duchateau J, Sacher F, Puyo S, Cochet H, Takigawa M, Denis A, Martin R, Derval N, Bordachar P, Ritter P, Ploux S, Pambrun T, Klotz N, Massoullié G, Pillois X, Dallet C, Schott JJ, Scouarnec S, Ackerman MJ, Tester D, Piot O, Pasquié JL, Leclerc C, Hermida JS, Gandjbakhch E, Maury P, Labrousse L, Coronel R, Jais P, Benoist D, Vigmond E, Potse M, Walton R, Nademanee K, Bernus O, Dubois R.. Localized structural alterations underlying a subset of unexplained sudden cardiac death. Circ Arrhythm Electrophysiol 2018;11:e006120. - PMC - PubMed
-
- Zaitsev AV, Berenfeld O, Mironov SF, Jalife J, Pertsov AM.. Distribution of excitation frequencies on the epicardial and endocardial surfaces of fibrillating ventricular wall of the sheep heart. Circ Res 2000;86:408–417. - PubMed
-
- Disertori M, Rigoni M, Pace N, Casolo G, Masè M, Gonzini L, Lucci D, Nollo G, Ravelli F.. Myocardial fibrosis assessment by LGE is a powerful predictor of ventricular tachyarrhythmias in ischemic and nonischemic LV dysfunction: a meta-analysis. JACC Cardiovasc Imaging 2016;9:1046–1055. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
