

The Impact of Glucocorticoid Co-Secretion in Primary Aldosteronism on Thyroid Autoantibody Titers During the Course of Disease
- PMID: 32403151
- PMCID: PMC7746512
- DOI: 10.1055/a-1164-1944
The Impact of Glucocorticoid Co-Secretion in Primary Aldosteronism on Thyroid Autoantibody Titers During the Course of Disease
Abstract
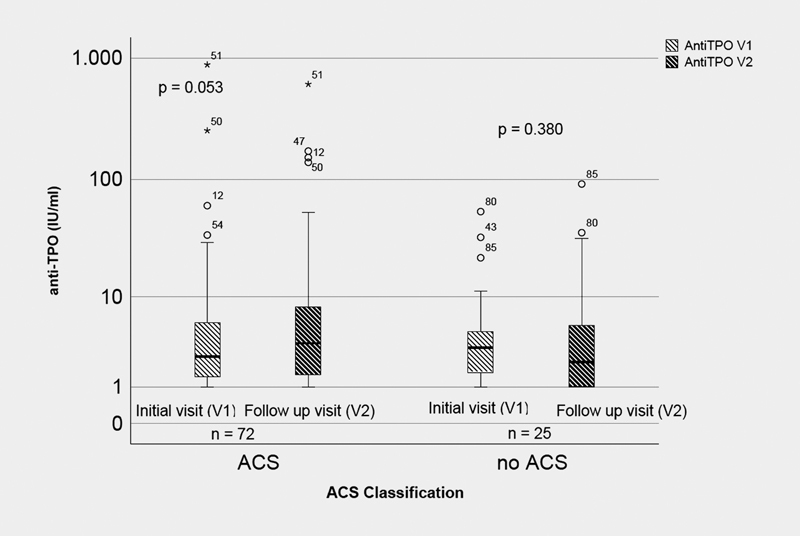
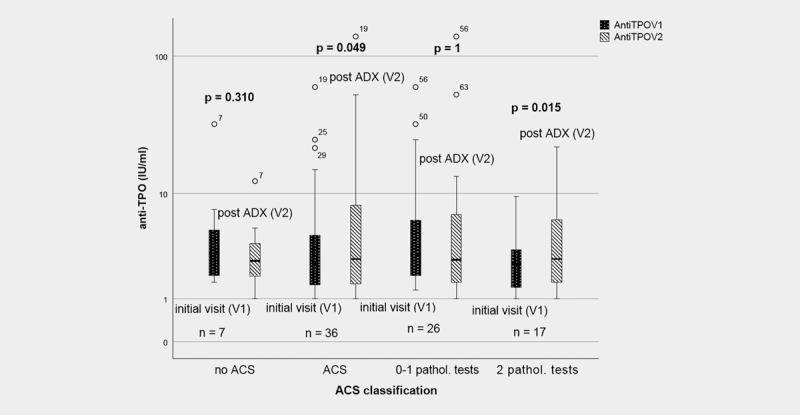
Excess aldosterone is associated with the increased risk of cardio-/cerebrovascular events as well as metabolic comorbidities not only due to its hypertensive effect but also due to its proinflammatory action. Autonomous cortisol secretion (ACS) in the setting of primary aldosteronism (PA) is known to worsen cardiovascular outcome and potentially exhibit immunosuppressive effects. The aim of this study was to determine the impact of ACS status in patients with PA on kinetics of thyroid autoantibodies (anti-TPO, anti-TG) pre and post therapy initiation. Ninety-seven PA patients (43 unilateral, 54 with bilateral PA) from the database of the German Conn's Registry were included. Anti-TPO and anti-TG levels were measured pre and 6-12 months post therapeutic intervention. Patients were assessed for ACS according to their 24- hour urinary cortisol excretion, late night salivary cortisol and low-dose dexamethasone suppression test. Abnormal test results in line with ACS were identified in 74.2% of patients with PA. Following adrenalectomy, significant increases in anti-TPO levels were observed in patients with at least one abnormal test (p = 0.049), adrenalectomized patients with at least two pathological ACS tests (p = 0.015) and adrenalectomized patients with pathologic dexamethasone suppression tests (p = 0.018). No antibody increases were observed in unilateral PA patients without ACS and in patients with bilateral PA receiving mineralocorticoid antagonist therapy (MRA). Our data are in line with an immunosuppressive effect of mild glucocorticoid excess in PA on thyroid autoantibody titers. This effect is uncovered by adrenalectomy, but not by MRA treatment.
© Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Rossi G P, Bernini G, Caliumi C et al. A prospective study of the prevalence of primary aldosteronism in 1125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–2300. - PubMed
-
- Funder J W, Carey R M, Mantero F et al. The management of primary aldosteronism: Case detection, diagnosis, and treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101:1889–1916. - PubMed
-
- Born-Frontsberg E, Reincke M, Rump L C et al. Cardiovascular and cerebrovascular comorbidities of hypokalemic and normokalemic primary aldosteronism: Results of the German Conn’s Registry. J Clin Endocrinol Metab. 2009;94:1125–1130. - PubMed
-
- Milliez P, Girerd X, Plouin P F et al. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005;45:1243–1248. - PubMed
-
- Quinkler M, Born-Frontsberg E, Fourkiotis V G. Comorbidities in primary aldosteronism. Horm Metab Res. 2010;42:429–434. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
