

A retrospective review of 10-year trends in general anesthesia for cesarean delivery at a university hospital: the impact of a newly launched team on obstetric anesthesia practice
- PMID: 32404093
- PMCID: PMC7371464
- DOI: 10.1186/s12913-020-05314-2
A retrospective review of 10-year trends in general anesthesia for cesarean delivery at a university hospital: the impact of a newly launched team on obstetric anesthesia practice
Abstract
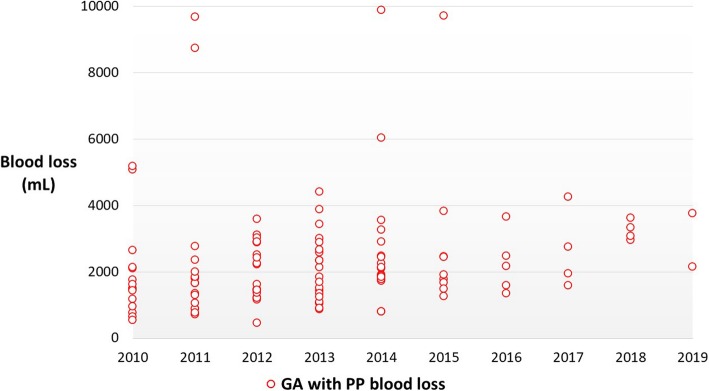
Background: The indications for general anesthesia (GA) in obstetric settings, which are determined in consideration of maternal and fetal outcome, could be affected by local patterns of clinical practice grounded in unique situations and circumstances that vary among medical institutions. Although the use of GA for cesarean delivery has become less common with more frequent adoption of neuraxial anesthesia, GA was previously chosen for pregnancy with placenta previa at our institution in case of unexpected massive hemorrhage. However, the situation has been gradually changing since formation of a team dedicated to obstetric anesthesia practice. Here, we report the results of a review of all cesarean deliveries performed under GA, and assess the impact of our newly launched team on trends in clinical obstetric anesthesia practice at our institution.
Methods: Our original database for obstetric GA during the period of 2010 to 2019 was analyzed. The medical records of all parturients who received GA for cesarean delivery were reviewed to collect detailed information. Interrupted time series analysis was used to evaluate the impact of the launch of our obstetric anesthesia team.
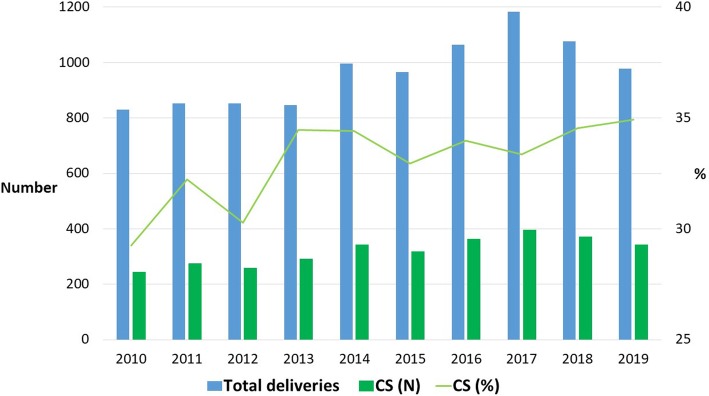
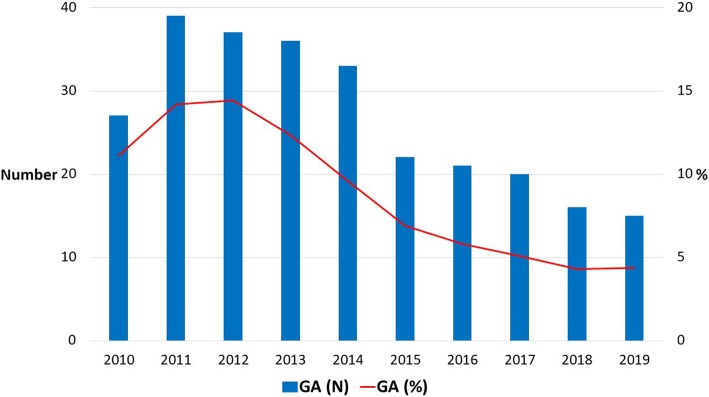
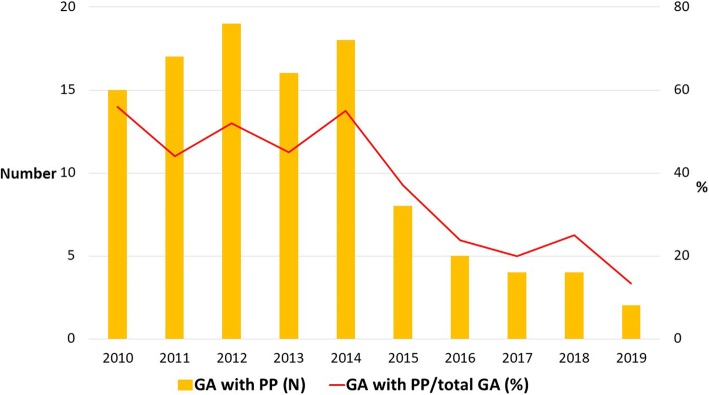
Results: As recently as 2014, more than 10% of cesarean deliveries were performed under GA, with placenta previa accounting for the main indication in elective and emergent cases. Our obstetric anesthesia team was formed in 2015 to serve as a communication bridge between the department of anesthesiology and the department of obstetrics. Since then, there has been a steady decline in the percentage of cesarean deliveries performed under GA, decreasing to a low of less than 5% in the latest 2 years. Interrupted time series analysis revealed a significant reduction in obstetric GA after 2015 (P = 0.04), which was associated with decreased use of GA for pregnancy with placenta previa. On the other hand, every year has seen a number of urgent cesarean deliveries requiring GA.
Conclusions: There has been a trend towards fewer obstetric GA since 2015. The optimized use of GA for cesarean delivery was made possible mainly through strengthened partnerships between anesthesiologists and obstetricians with the support of our obstetric anesthesia team.
Keywords: Cesarean delivery; General anesthesia; Multi-disciplinary collaboration; Obstetric anesthesia; Placenta previa.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Bloom SL, Spong CY, Weiner SJ, Landon MB, Rouse DJ, Varner MW, Moawad AH, Caritis SN, Harper M, Wapner RJ, Sorokin Y, Miodovnik M, O'Sullivan MJ, Sibai B, Langer O, Gabbe SG, National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network Complications of anesthesia for cesarean delivery. Obstet Gynecol. 2005;106(2):281–287. doi: 10.1097/01.AOG.0000171105.39219.55. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
