

Hypogeusia as the initial presenting symptom of COVID-19
- PMID: 32404376
- PMCID: PMC7228456
- DOI: 10.1136/bcr-2020-236080
Hypogeusia as the initial presenting symptom of COVID-19
Abstract
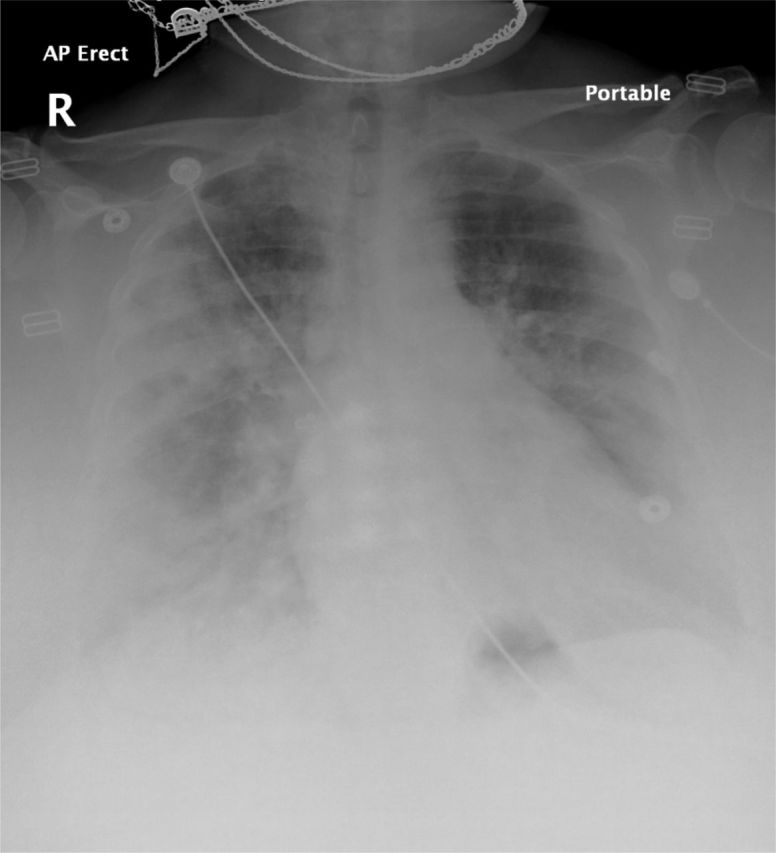
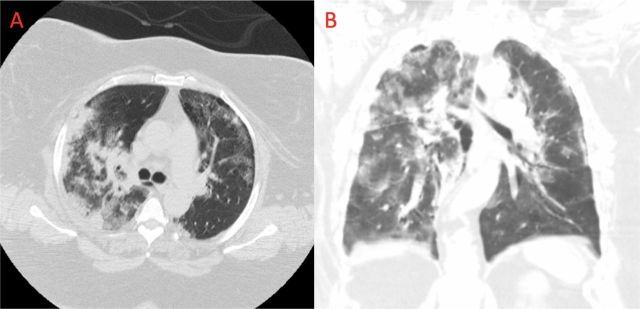
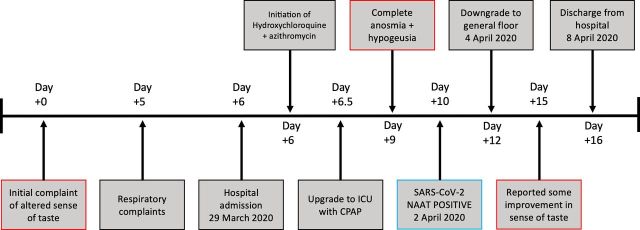
COVID-19 is the disease caused by the novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which first arose in Wuhan, China, in December 2019 and has since been declared a pandemic. The clinical sequelae vary from mild, self-limiting upper respiratory infection symptoms to severe respiratory distress, acute cardiopulmonary arrest and death. Otolaryngologists around the globe have reported a significant number of mild or otherwise asymptomatic patients with COVID-19 presenting with olfactory dysfunction. We present a case of COVID-19 resulting in intensive care unit (ICU) admission, presenting with the initial symptom of disrupted taste and flavour perception prior to respiratory involvement. After 4 days in the ICU and 6 days on the general medicine floor, our patient regained a majority of her sense of smell and was discharged with only lingering dysgeusia. In this paper, we review existing literature and the clinical course of SARS-CoV-2 in relation to the reported symptoms of hyposmia, hypogeusia and dysgeusia.
Keywords: adult intensive care; ear, nose and throat/otolaryngology; infectious diseases; mouth; pneumonia (respiratory medicine).
© BMJ Publishing Group Limited 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Shepherd GM. Neurogastronomy: how the brain creates flavor and why it matters. New York, NY: Columbia University Press, 2012.
-
- Johns Hopkins Coronavirus Resource Center COVID-19 MAP. Available: https://coronavirus.jhu.edu/map.html [Accessed 20 Apr 2020].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous