

Estimating the burden of SARS-CoV-2 in France
- PMID: 32404476
- PMCID: PMC7223792
- DOI: 10.1126/science.abc3517
Estimating the burden of SARS-CoV-2 in France
Erratum in
-
Erratum for the Report: "Estimating the burden of SARS-CoV-2 in France," by H. Salje, C. Tran Kiem, N. Lefrancq, N. Courtejoie, P. Bosetti, J. Paireau, A. Andronico, N. Hozé, J. Richet, C.-L. Dubost, Y. Le Strat, J. Lessler, D. Levy-Bruhl, A. Fontanet, L. Opatowski, P.-Y. Boelle, S. Cauchemez.Science. 2020 Jun 26;368(6498):eabd4246. doi: 10.1126/science.abd4246. Science. 2020. PMID: 32586992 Free PMC article. No abstract available.
Abstract
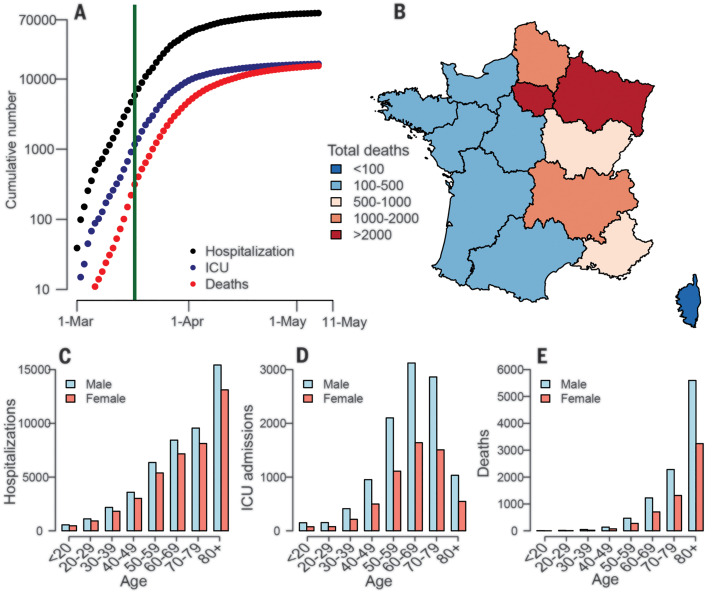
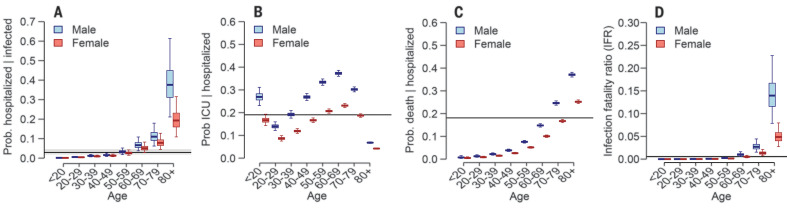
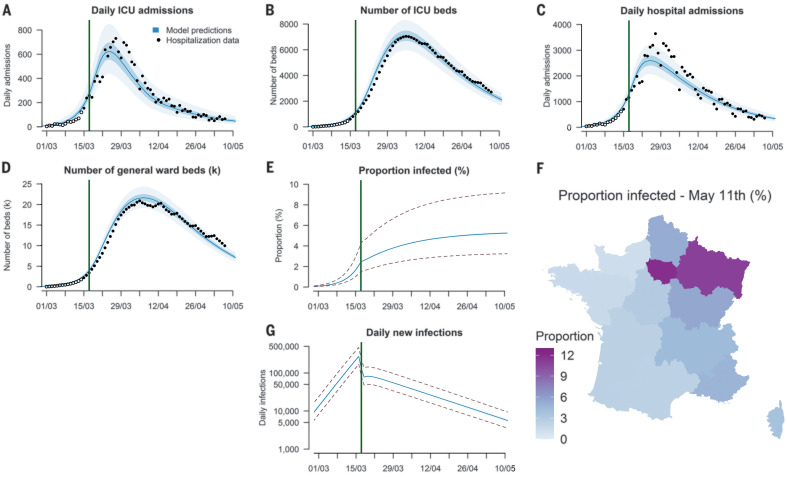
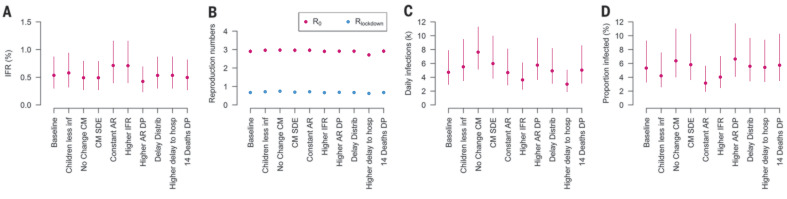
France has been heavily affected by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic and went into lockdown on 17 March 2020. Using models applied to hospital and death data, we estimate the impact of the lockdown and current population immunity. We find that 2.9% of infected individuals are hospitalized and 0.5% of those infected die (95% credible interval: 0.3 to 0.9%), ranging from 0.001% in those under 20 years of age to 8.3% in those 80 years of age or older. Across all ages, men are more likely to be hospitalized, enter intensive care, and die than women. The lockdown reduced the reproductive number from 2.90 to 0.67 (77% reduction). By 11 May 2020, when interventions are scheduled to be eased, we project that 3.5 million people (range: 2.1 million to 6.0 million), or 5.3% of the population (range: 3.3 to 9.3%), will have been infected. Population immunity appears to be insufficient to avoid a second wave if all control measures are released at the end of the lockdown.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
References
-
- Kraemer M. U. G., Yang C.-H., Gutierrez B., Wu C.-H., Klein B., Pigott D. M., du Plessis L., Faria N. R., Li R., Hanage W. P., Brownstein J. S., Layan M., Vespignani A., Tian H., Dye C., Pybus O. G., Scarpino S. V.; Open COVID-19 Data Working Group , The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 368, 493–497 (2020). 10.1126/science.abb4218 - DOI - PMC - PubMed
-
- Tian H., Liu Y., Li Y., Wu C.-H., Chen B., Kraemer M. U. G., Li B., Cai J., Xu B., Yang Q., Wang B., Yang P., Cui Y., Song Y., Zheng P., Wang Q., Bjornstad O. N., Yang R., Grenfell B. T., Pybus O. G., Dye C., An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science 368, 638–642 (2020). 10.1126/science.abb6105 - DOI - PMC - PubMed
-
- J. Lourenço, R. Paton, M. Ghafari, M.Kraemer, C. Thompson, P. Simmonds, P. Klenerman, S. Gupta, Fundamental principles of epidemic spread highlight the immediate need for large-scale serological surveys to assess the stage of the SARS-CoV-2 epidemic. medRxiv 2020.03.24.20042291 [Preprint]. 26 March 2020. 10.1101/2020.03.24.20042291. - DOI
-
- L. Bao, W. Deng, H. Gao, C. Xiao, J. Liu, J.Xue, Q. Lv, J. Liu, P. Yu, Y. Xu, F. Qi, Y. Qu, F. Li, Z. Xiang, H. Yu, S. Gong, M. Liu, G. Wang, S. Wang, Z. Song, W. Zhao, Y. Han, L. Zhao, X. Liu, Q. Wei, C.Qin, Reinfection could not occur in SARS-CoV-2 infected rhesus macaques. bioRxiv 2020.03.13.990226 [Preprint]. 14 March 2020. 10.1101/2020.03.13.990226. - DOI
-
- Lessler J., Salje H., Van Kerkhove M. D., Ferguson N. M., Cauchemez S., Rodriquez-Barraquer I., Hakeem R., Jombart T., Aguas R., Al-Barrak A., Cummings D. A. T.; MERS-CoV Scenario and Modeling Working Group , Estimating the severity and subclinical burden of Middle East respiratory syndrome coronavirus infection in the Kingdom of Saudi Arabia. Am. J. Epidemiol. 183, 657–663 (2016). 10.1093/aje/kwv452 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
