

ACTRIIA-Fc rebalances activin/GDF versus BMP signaling in pulmonary hypertension
- PMID: 32404506
- PMCID: PMC8259900
- DOI: 10.1126/scitranslmed.aaz5660
ACTRIIA-Fc rebalances activin/GDF versus BMP signaling in pulmonary hypertension
Abstract
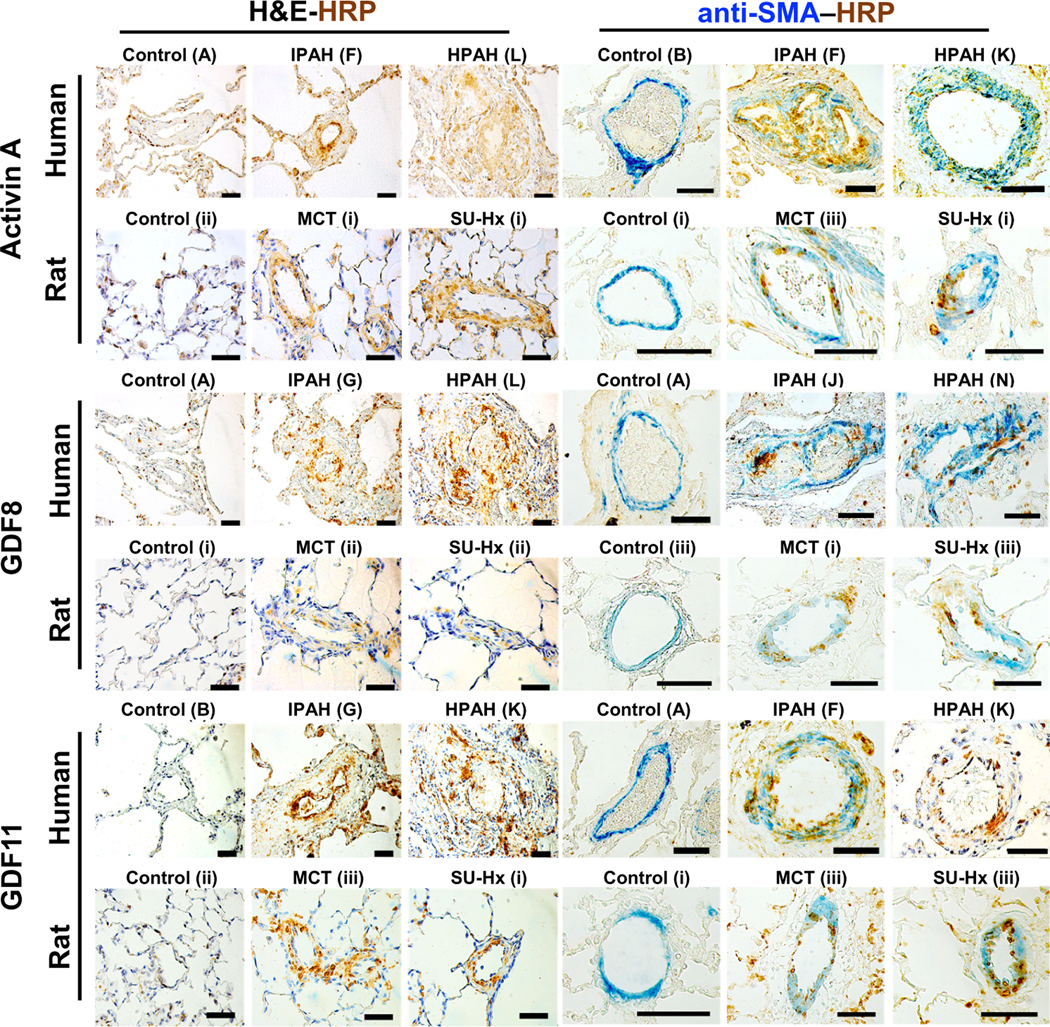
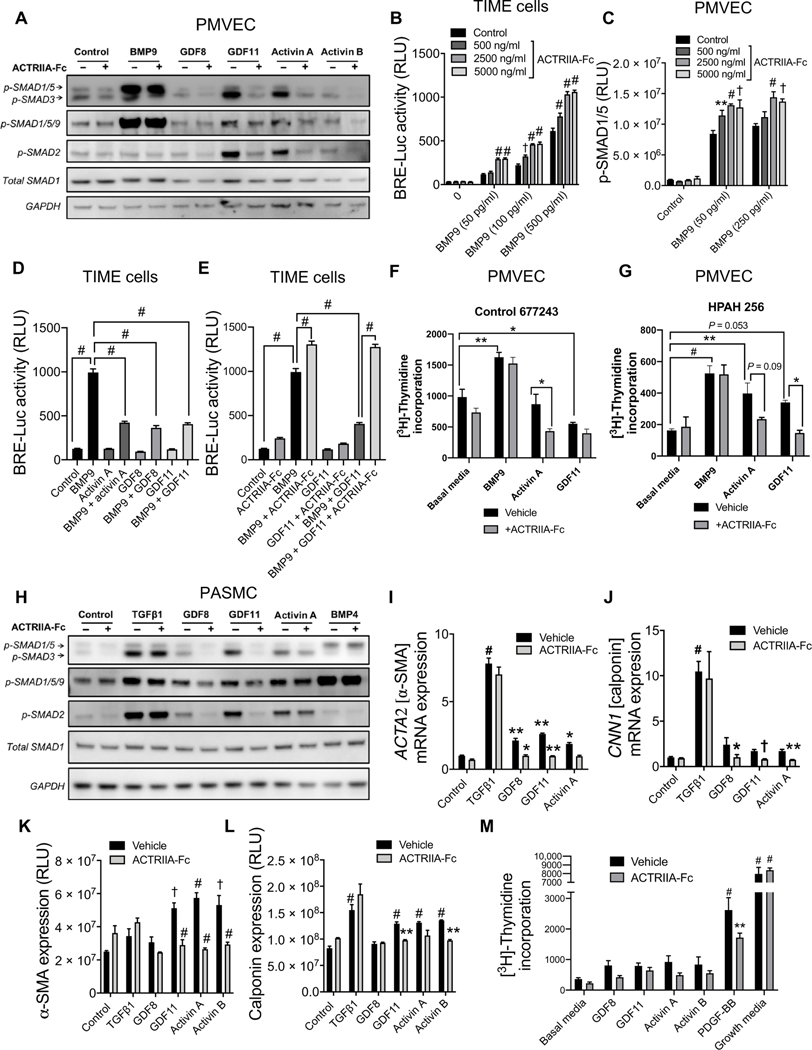
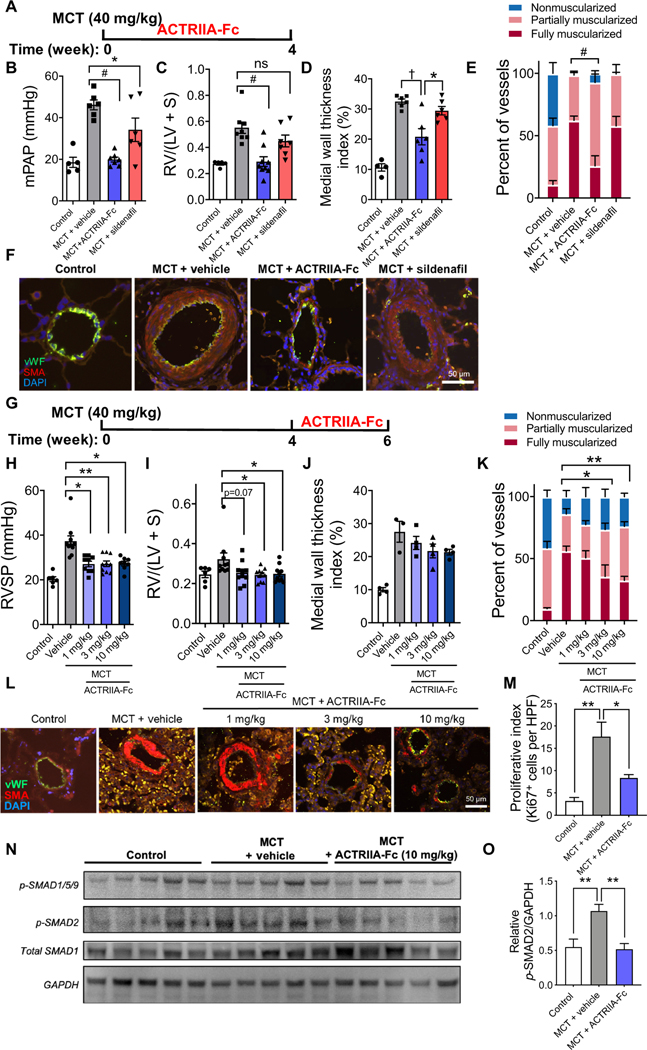
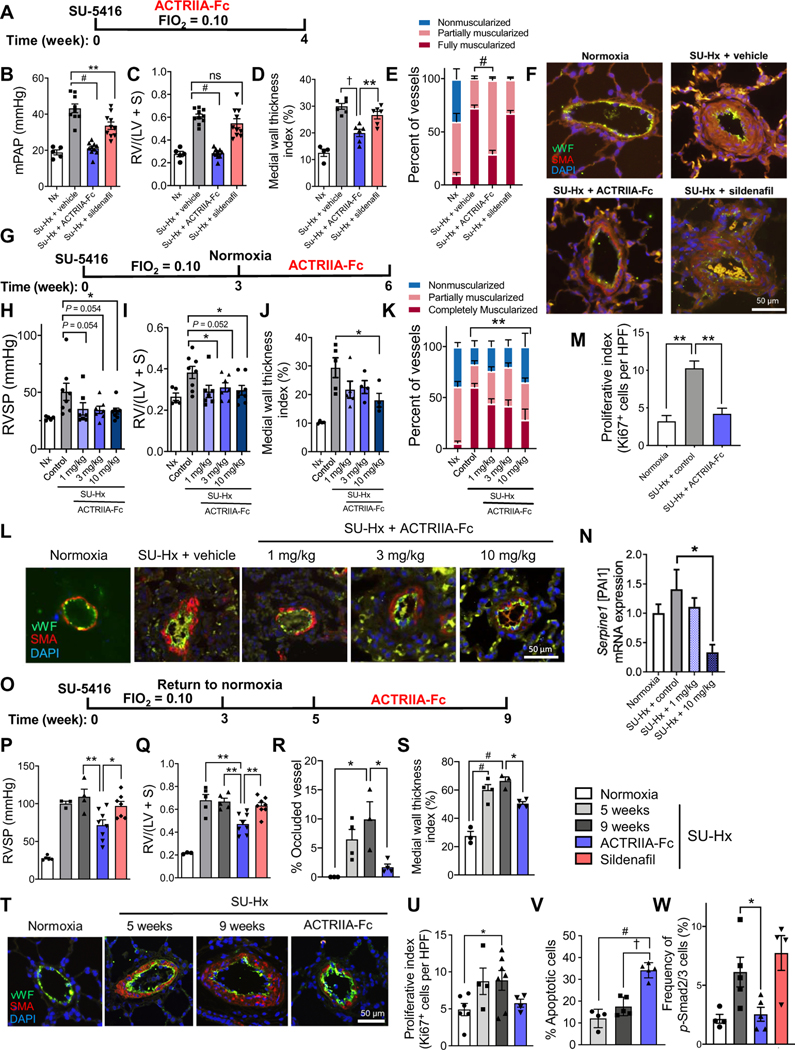
Human genetics, biomarker, and animal studies implicate loss of function in bone morphogenetic protein (BMP) signaling and maladaptive transforming growth factor-β (TGFβ) signaling as drivers of pulmonary arterial hypertension (PAH). Although sharing common receptors and effectors with BMP/TGFβ, the function of activin and growth and differentiation factor (GDF) ligands in PAH are less well defined. Increased expression of GDF8, GDF11, and activin A was detected in lung lesions from humans with PAH and experimental rodent models of pulmonary hypertension (PH). ACTRIIA-Fc, a potent GDF8/11 and activin ligand trap, was used to test the roles of these ligands in animal and cellular models of PH. By blocking GDF8/11- and activin-mediated SMAD2/3 activation in vascular cells, ACTRIIA-Fc attenuated proliferation of pulmonary arterial smooth muscle cells and pulmonary microvascular endothelial cells. In several experimental models of PH, prophylactic administration of ACTRIIA-Fc markedly improved hemodynamics, right ventricular (RV) hypertrophy, RV function, and arteriolar remodeling. When administered after the establishment of hemodynamically severe PH in a vasculoproliferative model, ACTRIIA-Fc was more effective than vasodilator in attenuating PH and arteriolar remodeling. Potent antiremodeling effects of ACTRIIA-Fc were associated with inhibition of SMAD2/3 activation and downstream transcriptional activity, inhibition of proliferation, and enhancement of apoptosis in the vascular wall. ACTRIIA-Fc reveals an unexpectedly prominent role of GDF8, GDF11, and activin as drivers of pulmonary vascular disease and represents a therapeutic strategy for restoring the balance between SMAD1/5/9 and SMAD2/3 signaling in PAH.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
References
-
- Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD, An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest 142, 448–456 (2012). - PubMed
-
- Soubrier F, Chung WK, Machado R, Grünig E, Aldred M, Geraci M, Loyd JE, Elliott CG, Trembath RC, Newman JH, Humbert M, Genetics and genomics of pulmonary arterial hypertension. J. Am. Coll. Cardiol 62, D13–D21 (2013). - PubMed
-
- Gräf S, Haimel M, Bleda M, Hadinnapola C, Southgate L, Li W, Hodgson J, Liu B, Salmon RM, Southwood M, Machado RD, Martin JM, Treacy CM, Yates K, Daugherty LC, Shamardina O, Whitehorn D, Holden S, Aldred M, Bogaard HJ, Church C, Coghlan G, Condliffe R, Corris PA, Danesino C, Eyries M, Gall H, Ghio S, Ghofrani H-A, Gibbs JSR, Girerd B, Houweling AC, Howard L, Humbert M, Kiely DG, Kovacs G, MacKenzie Ross RV, Moledina S, Montani D, Newnham M, Olschewski A, Olschewski H, Peacock AJ, Pepke-Zaba J, Prokopenko I, Rhodes CJ, Scelsi L, Seeger W, Soubrier F, Stein DF, Suntharalingam J, Swietlik EM, Toshner MR, van Heel DA, Noordegraaf AV, Waisfisz Q, Wharton J, Wort SJ, Ouwehand WH, Soranzo N, Lawrie A, Upton PD, Wilkins MR, Trembath RC, Morrell NW, Identification of rare sequence variation underlying heritable pulmonary arterial hypertension. Nat. Commun 9, 1416 (2018). - PMC - PubMed
-
- Thomas M, Docx C, Holmes AM, Beach S, Duggan N, England K, Leblanc C, Lebret C, Schindler F, Raza F, Walker C, Crosby A, Davies RJ, Morrell NW, Budd DC, Activin-like kinase 5 (ALK5) mediates abnormal proliferation of vascular smooth muscle cells from patients with familial pulmonary arterial hypertension and is involved in the progression of experimental pulmonary arterial hypertension induced by monocrotaline. Am. J. Pathol 174, 380–389 (2009). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
