

High systemic and tumor-associated IL-8 correlates with reduced clinical benefit of PD-L1 blockade
- PMID: 32405063
- PMCID: PMC8286544
- DOI: 10.1038/s41591-020-0860-1
High systemic and tumor-associated IL-8 correlates with reduced clinical benefit of PD-L1 blockade
Erratum in
-
Author Correction: High systemic and tumor-associated IL-8 correlates with reduced clinical benefit of PD-L1 blockade.Nat Med. 2021 Mar;27(3):560. doi: 10.1038/s41591-021-01246-4. Nat Med. 2021. PMID: 33547461 No abstract available.
Abstract
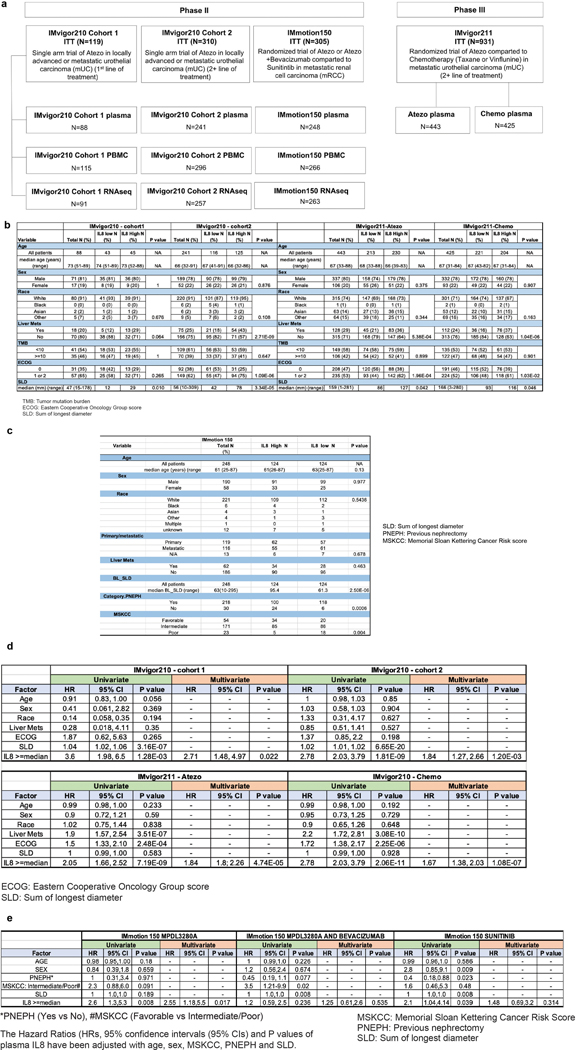
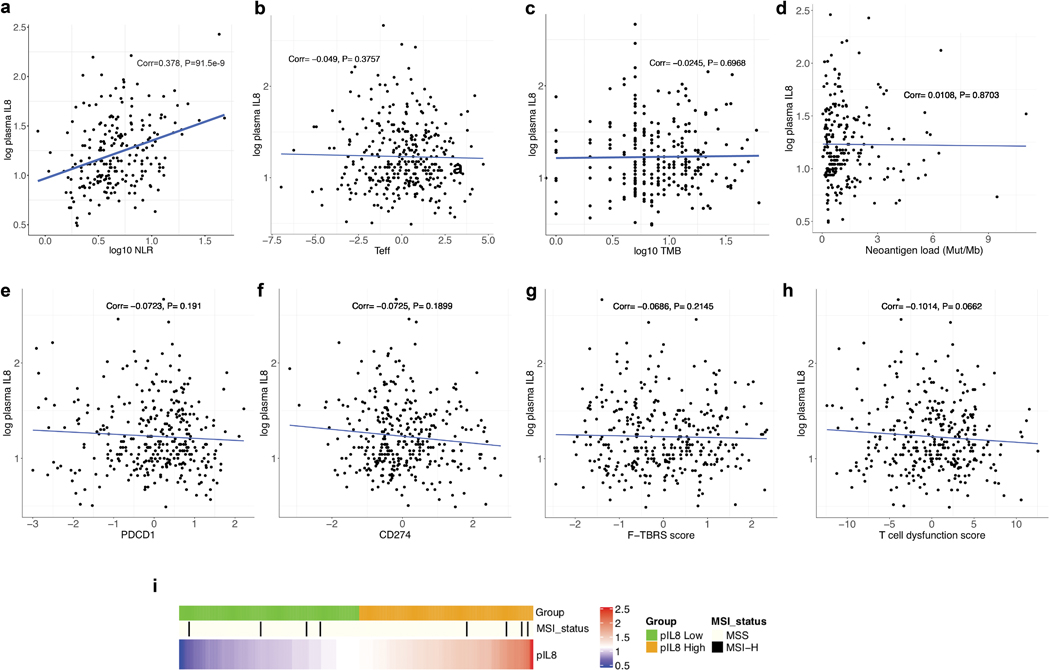
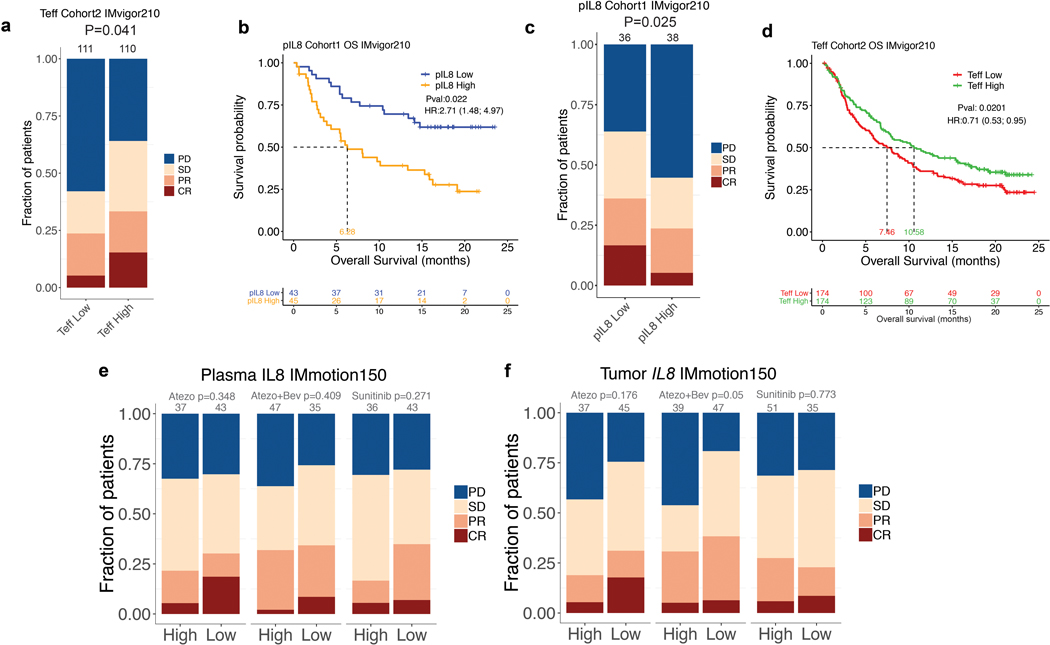
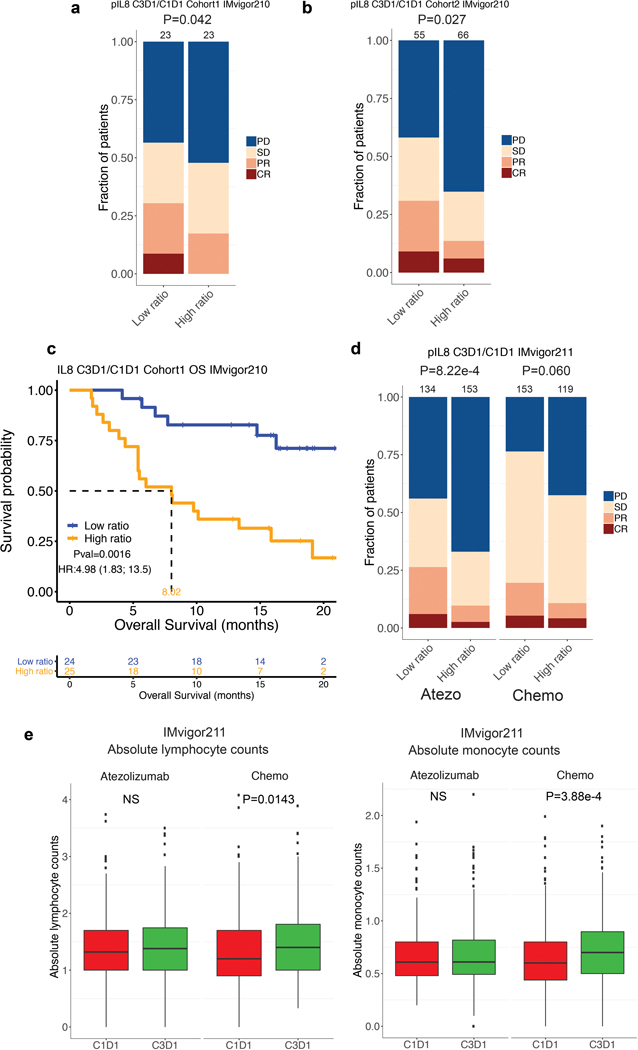
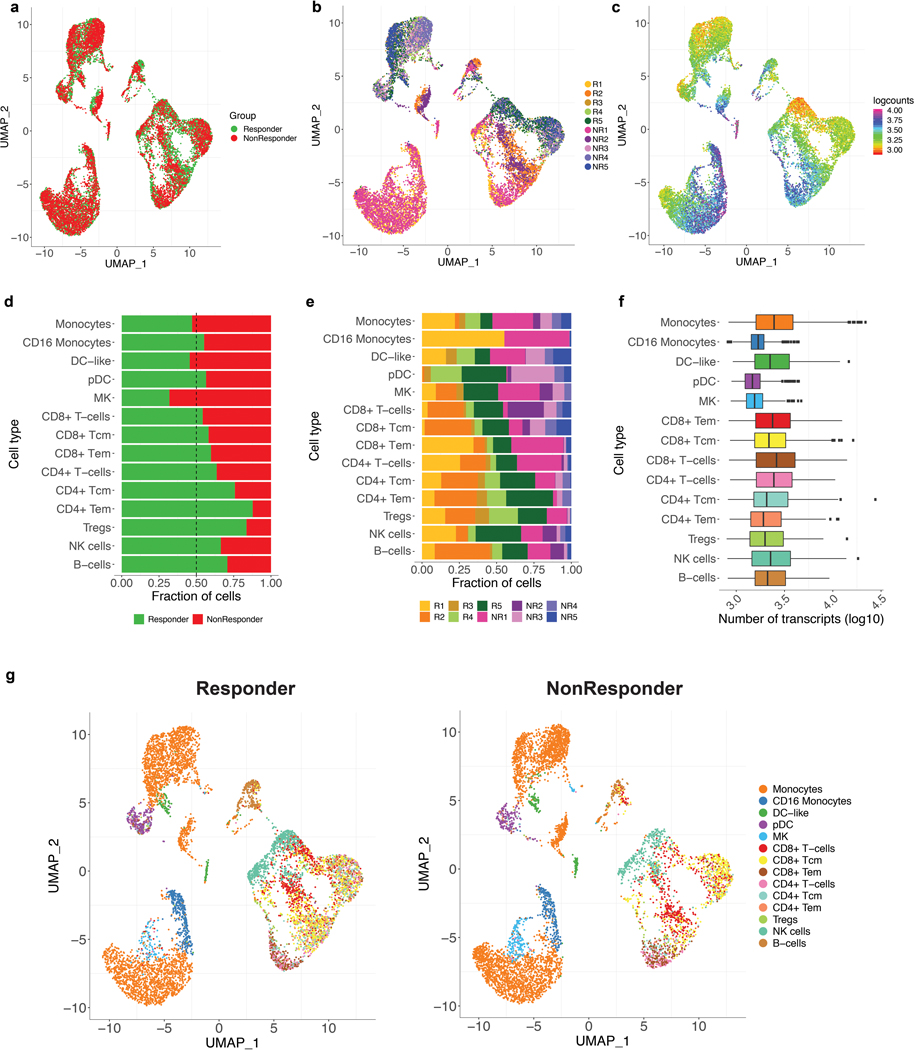
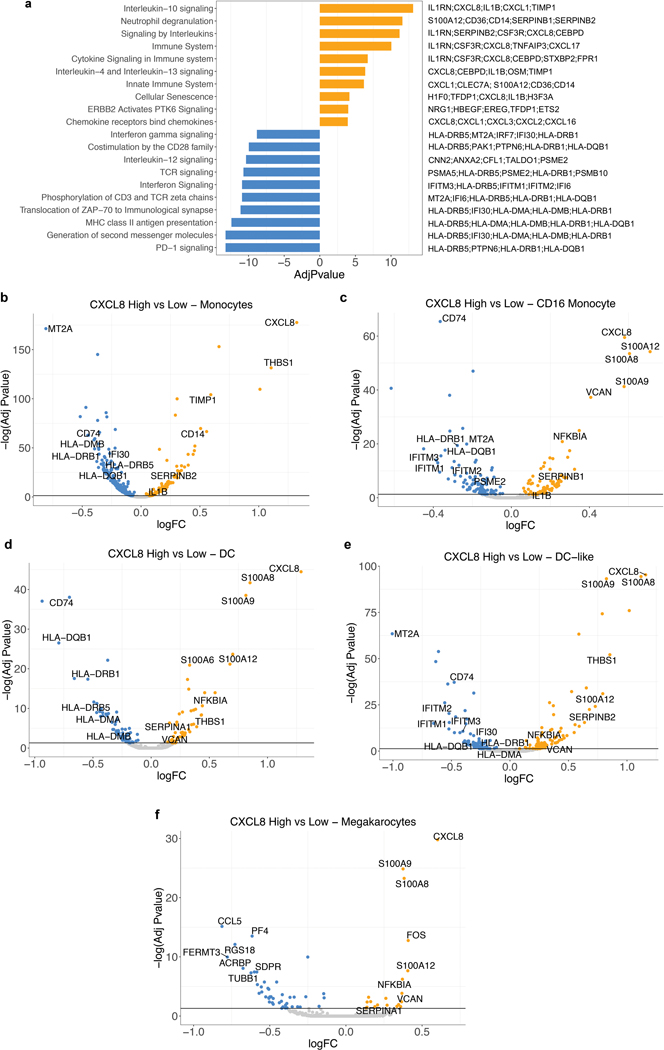
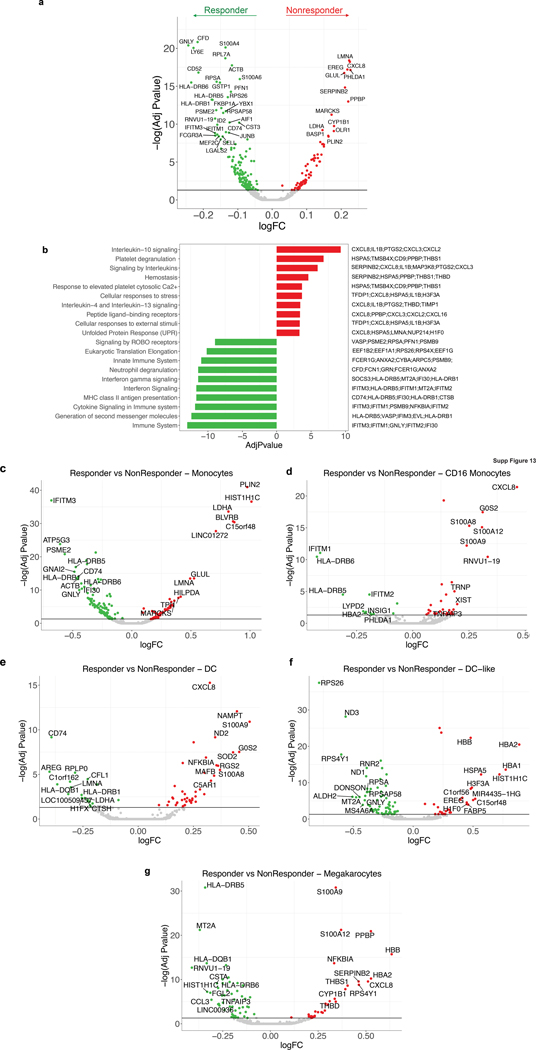
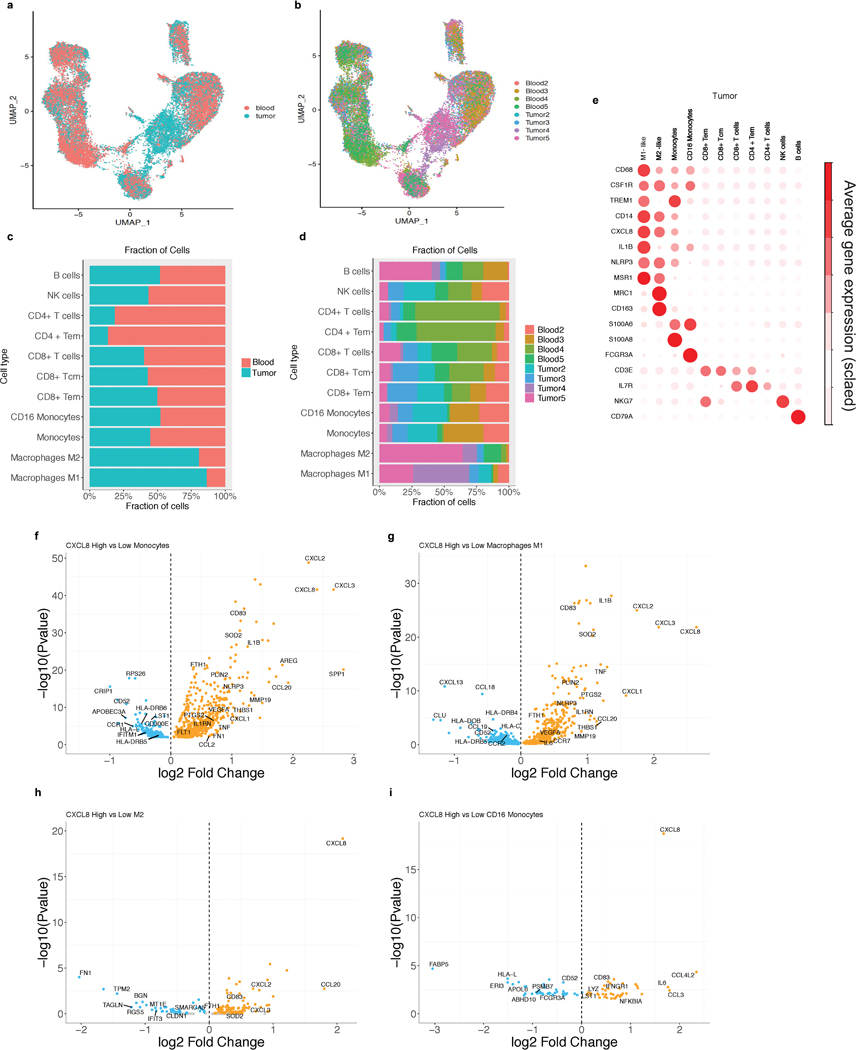
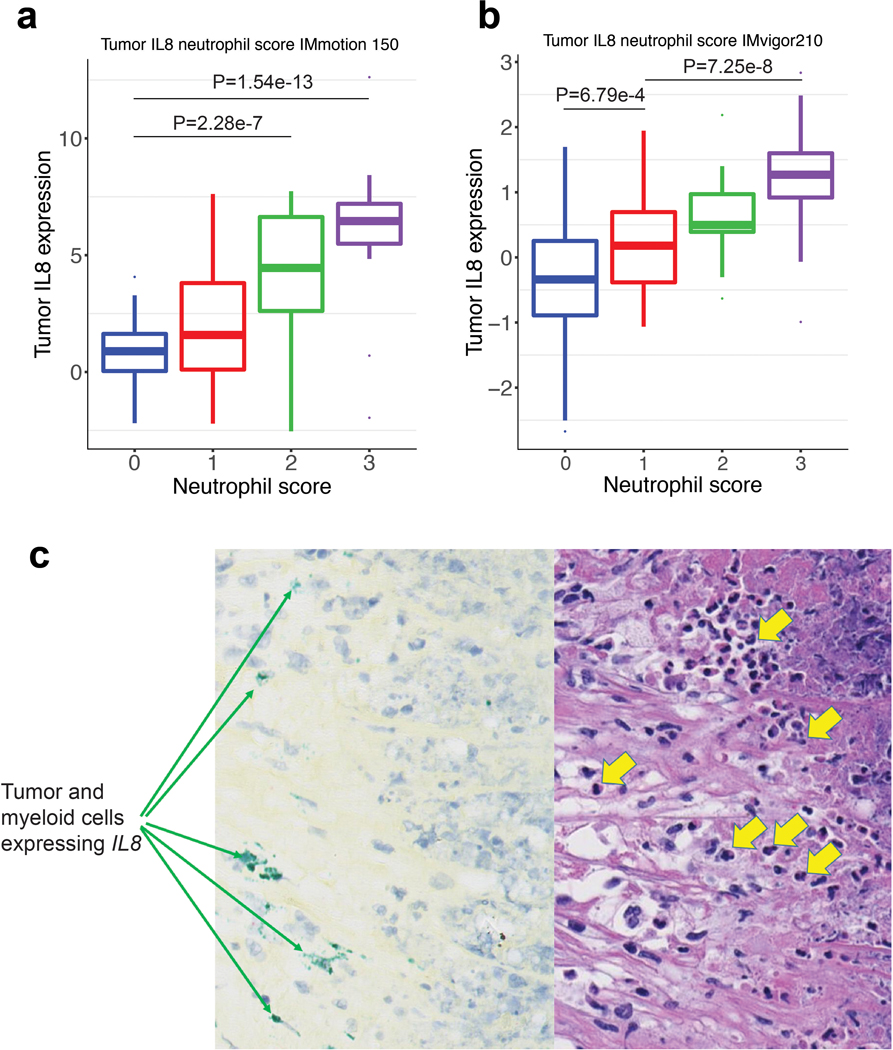
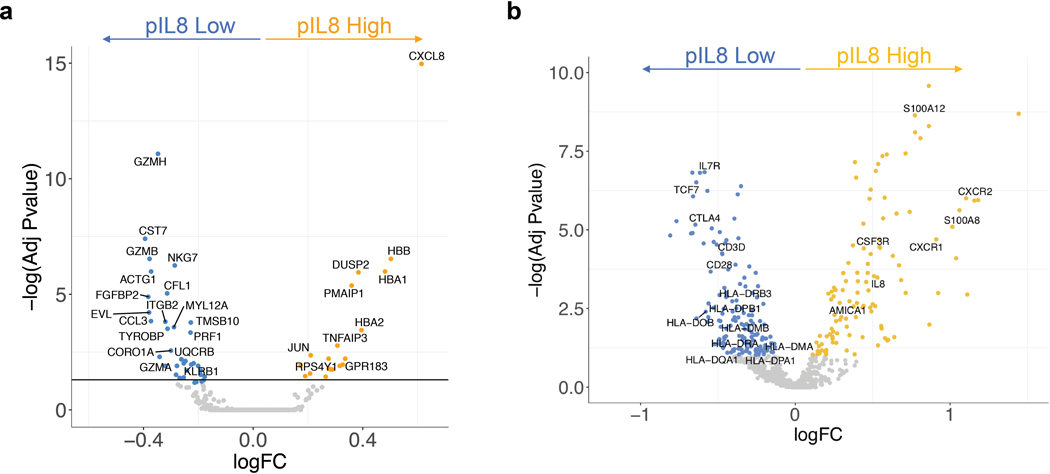
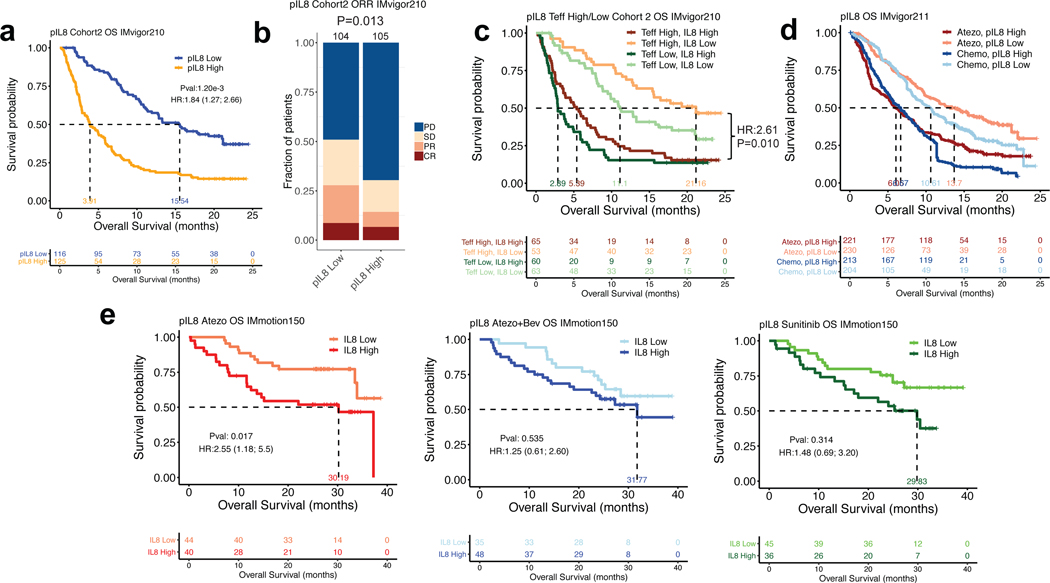
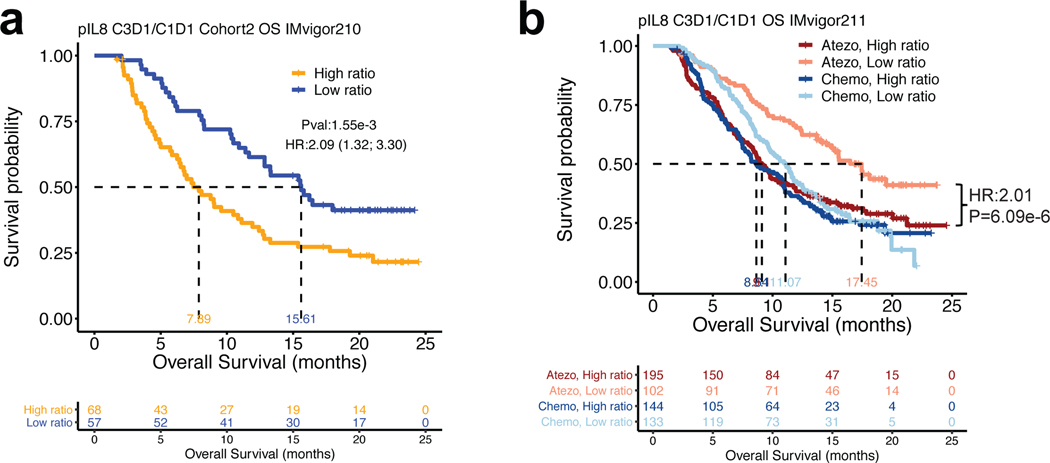
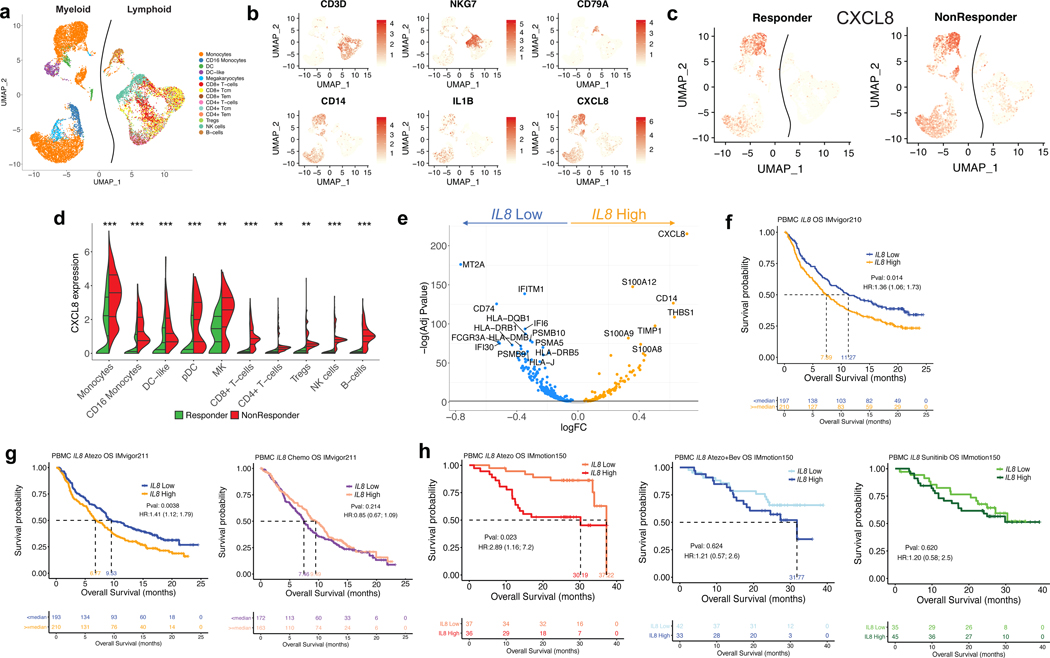
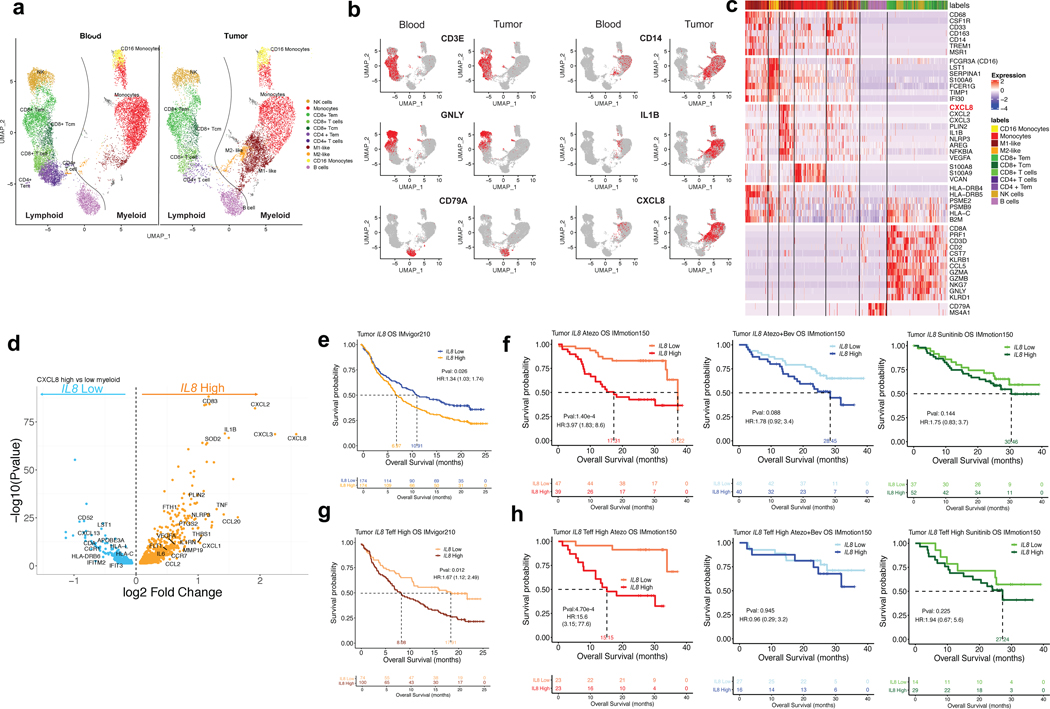
Although elevated plasma interleukin-8 (pIL-8) has been associated with poor outcome to immune checkpoint blockade 1, this has not been comprehensively evaluated in large randomized studies. Here we analyzed circulating pIL-8 and IL8 gene expression in peripheral blood mononuclear cells and tumors of patients treated with atezolizumab (anti-PD-L1 monoclonal antibody) from multiple randomized trials representing 1,445 patients with metastatic urothelial carcinoma (mUC) and metastatic renal cell carcinoma. High levels of IL-8 in plasma, peripheral blood mononuclear cells and tumors were associated with decreased efficacy of atezolizumab in patients with mUC and metastatic renal cell carcinoma, even in tumors that were classically CD8+ T cell inflamed. Low baseline pIL-8 in patients with mUC was associated with increased response to atezolizumab and chemotherapy. Patients with mUC who experienced on-treatment decreases in pIL-8 exhibited improved overall survival when treated with atezolizumab but not with chemotherapy. Single-cell RNA sequencing of the immune compartment showed that IL8 is primarily expressed in circulating and intratumoral myeloid cells and that high IL8 expression is associated with downregulation of the antigen-presentation machinery. Therapies that can reverse the impacts of IL-8-mediated myeloid inflammation will be essential for improving outcomes of patients treated with immune checkpoint inhibitors.
Figures
Comment in
-
IL-8 and cancer prognosis on immunotherapy.Nat Med. 2020 May;26(5):650-651. doi: 10.1038/s41591-020-0873-9. Nat Med. 2020. PMID: 32405061 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
