

doi: 10.22603/ssrr.2019-0043.
eCollection 2020.
A Crescent-Shaped Juxtafacet Cyst as a Rare Cause of High Thoracic Myelopathy with Partial Brown-Séquard's Syndrome
Affiliations
- PMID: 32405567
- PMCID: PMC7217681
- DOI: 10.22603/ssrr.2019-0043
Item in Clipboard
A Crescent-Shaped Juxtafacet Cyst as a Rare Cause of High Thoracic Myelopathy with Partial Brown-Séquard's Syndrome
Spine Surg Relat Res.
.
No abstract available
Keywords: high thoracic spine; intraspinal cyst; juxtafacet cyst; myelopathy.
Conflict of interest statement
Conflicts of Interest: The authors declare that there are no relevant conflicts of interest.
Figures

Preoperative MRIs. The right parasagittal T2-weighted (A), the axial T1-weighted (B), and the axial T2-weighted (C) MRIs show a well-defined, crescent-shaped, cystic mass lesion in the epidural space, located right posterolaterally in the canal, adjacent to the right T2-T3 facet joint (i.e., juxtafacet cyst [JFC], arrows). Note the joint effusion in the right T2-T3 facet joint space shown by the axial MRIs (arrow heads).
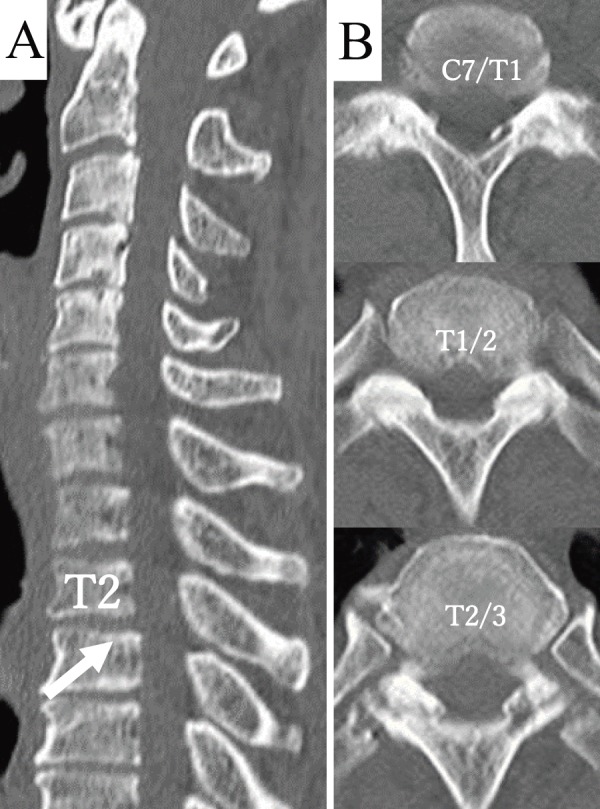
Preoperative CT scans. The midsagittal reformatted CT image (A) shows a reduced cervical lordosis and mild spondylolisthesis of T2 on T3 (arrow). The axial CT images (B) indicate the severely degenerated facet joints bilaterally at C7-T1 through T2-T3 with spontaneous facet fusion at C7-T1 and T1-T2.

Intraoperative microscopic views. Operative photographs following laminectomy with medial facetectomies at T2-T3 level on both sides and the removal of the ligamentum flavum, showing the JFC adjacent to the right T2-T3 facet joint (arrows) under a low (A) and a high magnification (B) of the microscope. Firm adhesion between the cyst wall and the dura (C) was dissected off with mostly a blunt microdissection resulting in a complete cyst removal (D).

Postoperative MRIs at 2 months. Midsagittal T2-weighted (A), axial T1-weighted (B), and axial T2-weighted (C) MRIs, showing complete cyst removal with adequate decompression of the spinal cord.
References
-
- Finkelstein SD, Sayegh R, Watson P, et al. Juxta-facet cysts. Report of two cases and review of clinicopathologic features. Spine (Phila Pa 1976). 1993;18(6):779-82. - PubMed
-
- Cohen-Gadol AA, White JB, Lynch JJ, et al. Synovial cysts of the thoracic spine. J Neurosurg Spine. 2004;1(1):52-7. - PubMed
-
- Howington JU, Connolly ES, Voorhies RM. Intraspinal synovial cysts: 10-year experience at the ochsner clinic. J Neurosurg. 1999;91:193-9. - PubMed
-
- Daentzer D, Stüder D. Thoracic juxtafacet cyst (JFC) as a rare cause of myelopathy--an additional reference to support the instability theory. Joint Bone Spine. 2010;77(2):178-80. - PubMed
LinkOut - more resources
Full Text Sources