

Prevention and management of COVID-19 among patients with diabetes: an appraisal of the literature
- PMID: 32405783
- PMCID: PMC7220850
- DOI: 10.1007/s00125-020-05164-x
Prevention and management of COVID-19 among patients with diabetes: an appraisal of the literature
Abstract
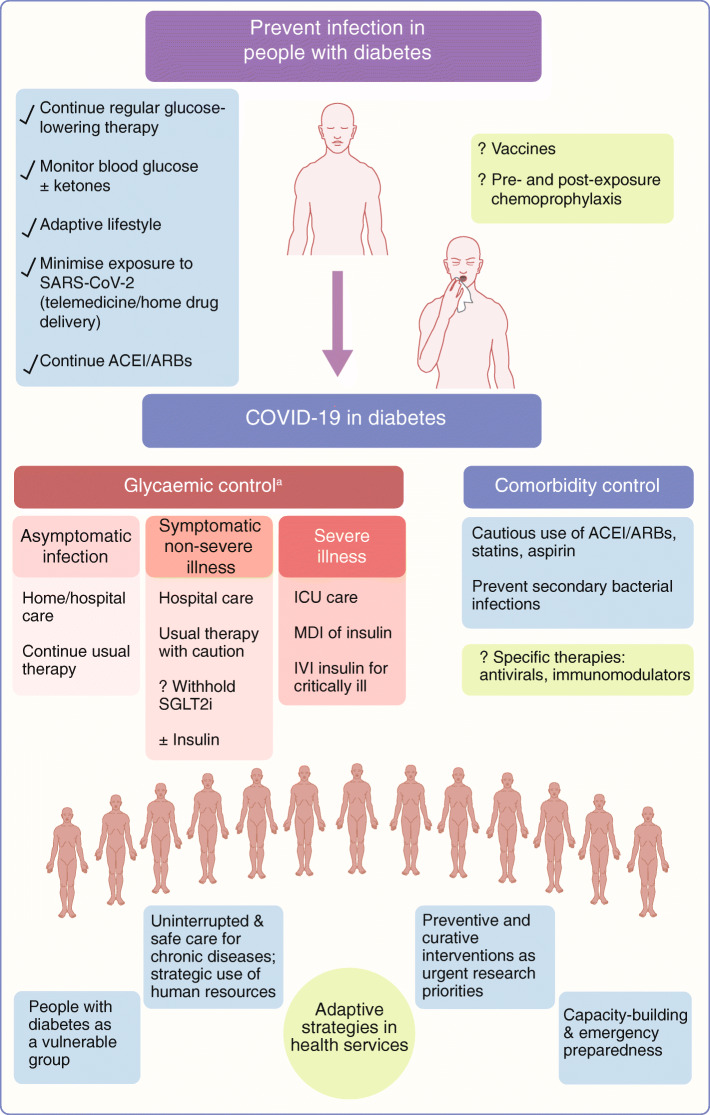
The coronavirus disease 2019 (COVID-19) pandemic has emerged as one of the greatest challenges faced by humankind in the recent past. People with diabetes and related comorbidities are at increased risk of its complications and of COVID-19-related death. Older age, multi-morbidity, hyperglycaemia, cardiac injury and severe inflammatory response are predictors of poor outcome. The complex interplay between COVID-19, diabetes and the effects of related therapies is being explored. Most patients experience a mild illness with COVID-19, while people with diabetes are at increased risk of severe disease. Optimising glycaemic control and adopting measures to prevent disease spread are critical aspects. The management of mild disease is supportive, while very many immunomodulatory and antiviral therapies are being investigated for the treatment of severe disease. Several of these agents have specific considerations for use in people with diabetes. Since mass population lockdowns are considered a key step in controlling disease spread, it follows that, in addition to the direct vulnerability to severe COVID-19, people with diabetes can be affected by limited access to healthcare, insulin, other medications and blood glucose monitoring equipment. Measures to prevent disease spread at the individual and community level are the key to mitigating the rapidly escalating pandemic, while agents for chemoprophylaxis and vaccines are being explored. People with diabetes should be recognised as a vulnerable group for complicated disease and are at risk during times of disturbed social systems. Strategies are needed to safeguard the health of patients with diabetes during the pandemic. This review summarises the current knowledge and perceived challenges for prevention and management of COVID-19 in people with diabetes.
Keywords: COVID-19; Coronavirus; Diabetes; SARS-CoV-2.
Figures

References
-
- Woldometer (2020) COVID-19 coronavirus pandemic. Available from https://www.worldometers.info/coronavirus/. Accessed 13 Apr 2020
-
- World Health Organization HO (2020) Coronavirus disease 2019 (COVID-19) situation report–62. Available from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed 22 Mar 2020
-
- World Health Organization (2020) Report of the WHO–China Joint Mission on coronavirus disease 2019 (COVID-19). Available from https://www.who.int/publications-detail/report-of-the-who-china-joint-mi...). Accessed 20 Apr 2020
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
