

Sepsis at ICU admission does not decrease 30-day survival in very old patients: a post-hoc analysis of the VIP1 multinational cohort study
- PMID: 32406016
- PMCID: PMC7221097
- DOI: 10.1186/s13613-020-00672-w
Sepsis at ICU admission does not decrease 30-day survival in very old patients: a post-hoc analysis of the VIP1 multinational cohort study
Abstract
Background: The number of intensive care patients aged ≥ 80 years (Very old Intensive Care Patients; VIPs) is growing. VIPs have high mortality and morbidity and the benefits of ICU admission are frequently questioned. Sepsis incidence has risen in recent years and identification of outcomes is of considerable public importance. We aimed to determine whether VIPs admitted for sepsis had different outcomes than those admitted for other acute reasons and identify potential prognostic factors for 30-day survival.
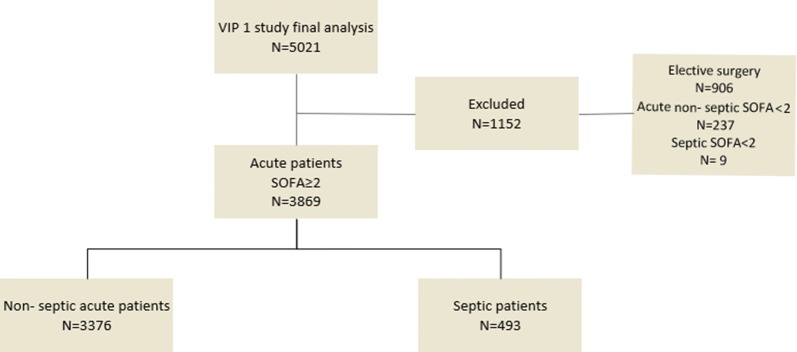
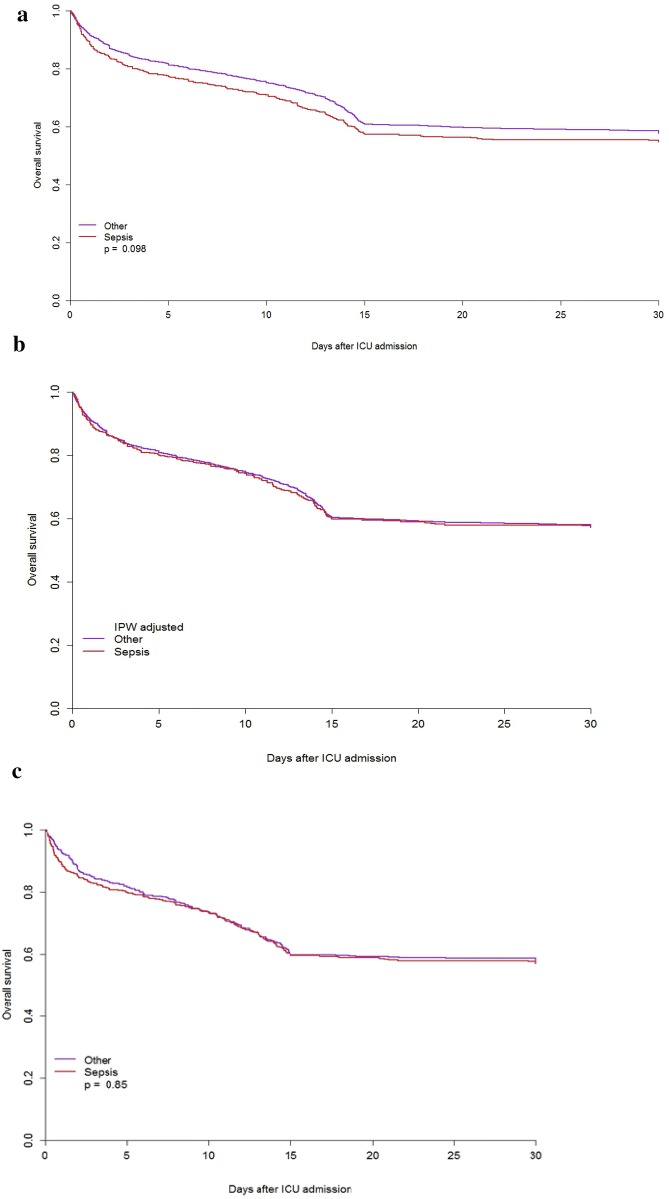
Results: This prospective study included VIPs with Sequential Organ Failure Assessment (SOFA) scores ≥ 2 acutely admitted to 307 ICUs in 21 European countries. Of 3869 acutely admitted VIPs, 493 (12.7%) [53.8% male, median age 83 (81-86) years] were admitted for sepsis. Sepsis was defined according to clinical criteria; suspected or demonstrated focus of infection and SOFA score ≥ 2 points. Compared to VIPs admitted for other acute reasons, VIPs admitted for sepsis were younger, had a higher SOFA score (9 vs. 7, p < 0.0001), required more vasoactive drugs [82.2% vs. 55.1%, p < 0.0001] and renal replacement therapies [17.4% vs. 9.9%; p < 0.0001], and had more life-sustaining treatment limitations [37.3% vs. 32.1%; p = 0.02]. Frailty was similar in both groups. Unadjusted 30-day survival was not significantly different between the two groups. After adjustment for age, gender, frailty, and SOFA score, sepsis had no impact on 30-day survival [HR 0.99 (95% CI 0.86-1.15), p = 0.917]. Inverse-probability weight (IPW)-adjusted survival curves for the first 30 days after ICU admission were similar for acute septic and non-septic patients [HR: 1.00 (95% CI 0.87-1.17), p = 0.95]. A matched-pair analysis in which patients with sepsis were matched with two control patients of the same gender with the same age, SOFA score, and level of frailty was also performed. A Cox proportional hazard regression model stratified on the matched pairs showed that 30-day survival was similar in both groups [57.2% (95% CI 52.7-60.7) vs. 57.1% (95% CI 53.7-60.1), p = 0.85].
Conclusions: After adjusting for organ dysfunction, sepsis at admission was not independently associated with decreased 30-day survival in this multinational study of 3869 VIPs. Age, frailty, and SOFA score were independently associated with survival.
Keywords: Intensive care; Mortality; Outcome; Sepsis; Severity of illness; Survival; Very old.
Conflict of interest statement
None of the authors have competing interests; all authors have read the current “Instructions to authors” and accept the conditions posed therein. This manuscript is original and has not been and will not be simultaneously submitted elsewhere for publication. None of the material from this study is included in another manuscript, has been published previously, or has been posted on the internet.
Figures
References
LinkOut - more resources
Full Text Sources
