

Systematic review: medical therapy for fibrostenosing Crohn's disease
- PMID: 32406116
- PMCID: PMC7777136
- DOI: 10.1111/apt.15750
Systematic review: medical therapy for fibrostenosing Crohn's disease
Abstract
Background: Medical therapy and/or endoscopic balloon dilation with intralesional therapies are options for the treatment of small bowel fibrostenotic Crohn's disease (CD).
Aim: To perform a systematic review summarising evidence for efficacy of systemic and endoscopic intralesional medical therapy in established small bowel strictures in adult CD patients.
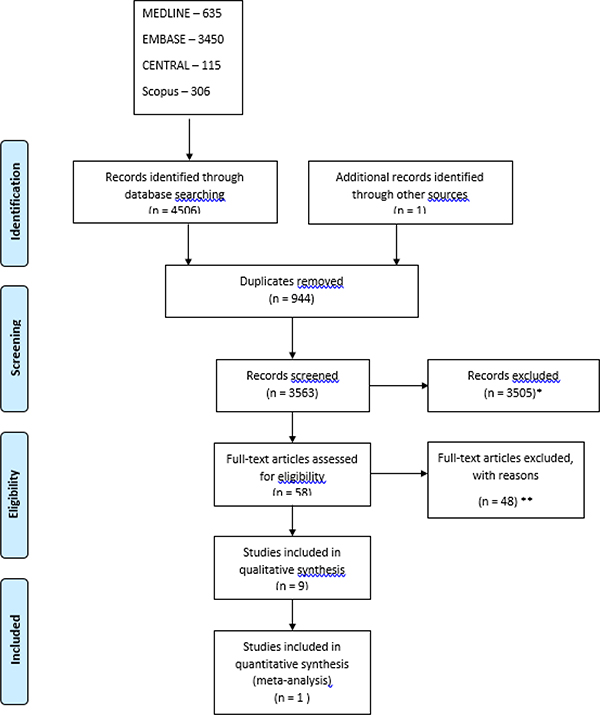
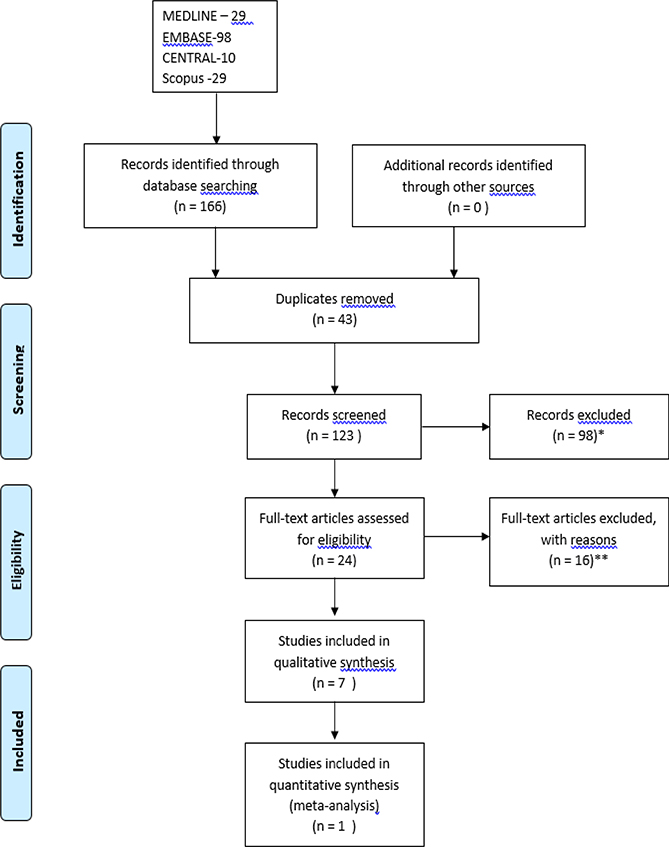
Methods: A systematic search of MEDLINE, EMBASE, CENTRAL and Scopus was conducted. Primary outcomes were rates of surgical resection and repeat endoscopic dilation. Pooled event rates from random effects models across studies with 95% confidence intervals were reported.
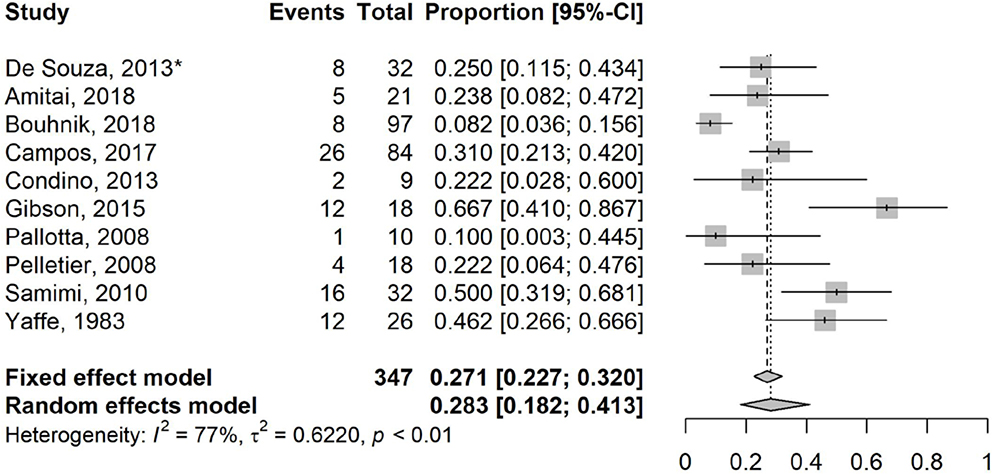
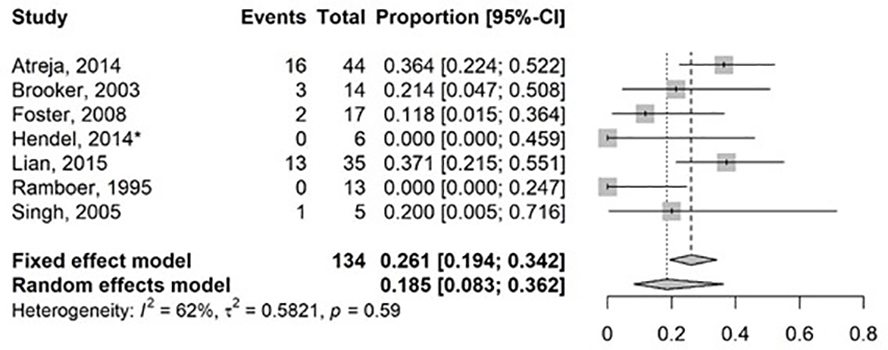
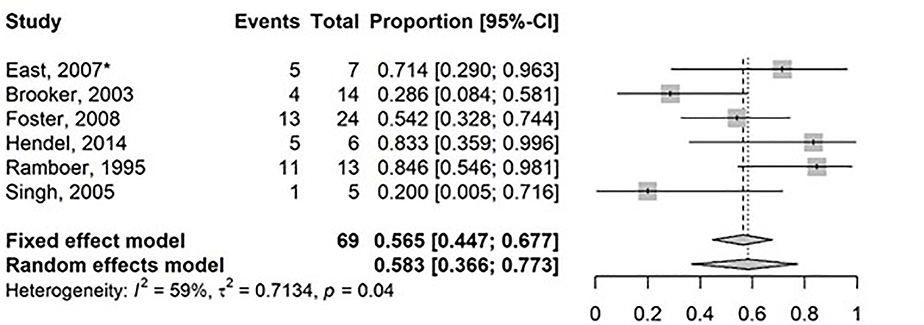
Results: Ten studies describing systemic medical therapy and eight studies of intralesional injection were included. One randomised controlled trial each for systemic therapy and intrastricture injection were identified. Only observational studies were found for systemic biologic therapies, which exclusively included tumour necrosis factor (TNF) antagonists, while intralesional therapies all involved corticosteroids except for one study that evaluated infliximab. Pooled event rates for surgical resection after systemic and intralesional therapy were 28.3% (95% CI: 18.2%-41.3%) and 18.5% (95% CI: 8.3%-36.2%), respectively over a median follow-up of 23 months (range 5.5-105.8), and 21.8 months (range 5-47). Risk of repeat endoscopic balloon dilation in those with intralesional therapy was 58.3% (95% CI: 36.6%-77.3%) over a median follow-up of 21.8 months (range 5-47).
Conclusions: There are no favoured therapies for patients with stricturing small bowel CD. Data are lacking for ustekinumab and vedolizumab. No endoscopic intralesional medications provided a clear benefit for prevention of repeat EBD or surgery.
© 2020 John Wiley & Sons Ltd.
Conflict of interest statement
ii. Brandon Baraty, Helen Lee Robertson, Alexis Filyk, Tak Fung, and Jean-Paul Achkar have no conflicts of interests to declare.
Figures
Similar articles
-
Efficacy of drug and endoscopic treatment of Crohn's disease strictures: A systematic review.J Gastroenterol Hepatol. 2021 Feb;36(2):344-361. doi: 10.1111/jgh.15330. Epub 2020 Dec 27. J Gastroenterol Hepatol. 2021. PMID: 33150989
-
Analysis of the Risk Factors of Surgery after Endoscopic Balloon Dilation for Small Intestinal Strictures in Crohn's Disease Using Double-balloon Endoscopy.Intern Med. 2017 Sep 1;56(17):2245-2252. doi: 10.2169/internalmedicine.8224-16. Epub 2017 Aug 10. Intern Med. 2017. PMID: 28794359 Free PMC article.
-
Natural history, diagnosis and treatment approach to fibrostenosing Crohn's disease.United European Gastroenterol J. 2020 Apr;8(3):263-270. doi: 10.1177/2050640620901960. Epub 2020 Jan 14. United European Gastroenterol J. 2020. PMID: 32213020 Free PMC article. Review.
-
Endoscopic management of Crohn's strictures.World J Gastroenterol. 2018 May 7;24(17):1859-1867. doi: 10.3748/wjg.v24.i17.1859. World J Gastroenterol. 2018. PMID: 29740201 Free PMC article. Review.
-
Systematic review with meta-analysis: efficacy of balloon-assisted enteroscopy for dilation of small bowel Crohn's disease strictures.Aliment Pharmacol Ther. 2020 Oct;52(7):1104-1116. doi: 10.1111/apt.16049. Epub 2020 Aug 19. Aliment Pharmacol Ther. 2020. PMID: 32813282 Free PMC article.
Cited by
-
Early Laparoscopic Ileal Resection for Localized Ileocecal Crohn's Disease: Hard Sell or a Revolutionary New Norm?Inflamm Intest Dis. 2021 May 19;7(1):13-20. doi: 10.1159/000515959. eCollection 2022 Jan. Inflamm Intest Dis. 2021. PMID: 35224013 Free PMC article. Review.
-
Increasing Rates of Bowel Resection Surgery for Stricturing Crohn's Disease in the Biologic Era.Inflamm Bowel Dis. 2025 Apr 10;31(4):935-943. doi: 10.1093/ibd/izae113. Inflamm Bowel Dis. 2025. PMID: 38795051 Free PMC article.
-
Therapeutic Targeting of Intestinal Fibrosis in Crohn's Disease.Cells. 2022 Jan 26;11(3):429. doi: 10.3390/cells11030429. Cells. 2022. PMID: 35159238 Free PMC article. Review.
-
Surgery for Crohn's disease: upfront or last resort?Gastroenterol Rep (Oxf). 2022 Nov 9;10:goac063. doi: 10.1093/gastro/goac063. eCollection 2022. Gastroenterol Rep (Oxf). 2022. PMID: 36381220 Free PMC article. Review.
-
Ustekinumab is effective against ulcerative colitis with intestinal stenosis: A case report.Medicine (Baltimore). 2022 Oct 21;101(42):e31213. doi: 10.1097/MD.0000000000031213. Medicine (Baltimore). 2022. PMID: 36281114 Free PMC article.
References
-
- Rieder F, Latella G, Magro F, et al. European Crohn’s and Colitis Organisation Topical Review on Prediction, Diagnosis and Management of Fibrostenosing Crohn’s Disease. J. Crohn’s Colitis 2016;10:873–885. - PubMed
-
- Lazarev M, Uliman T, Schraut WH, et al. Small bowel resection rates in Crohn’s disease and the indication for surgery over time: Experience from a large tertiary care center. Inflamm. Bowel Dis. 2010;16:830–835. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical