

Automatic Triage of 12-Lead ECGs Using Deep Convolutional Neural Networks
- PMID: 32406296
- PMCID: PMC7660886
- DOI: 10.1161/JAHA.119.015138
Automatic Triage of 12-Lead ECGs Using Deep Convolutional Neural Networks
Abstract
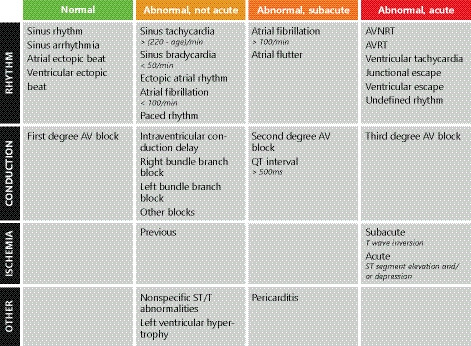
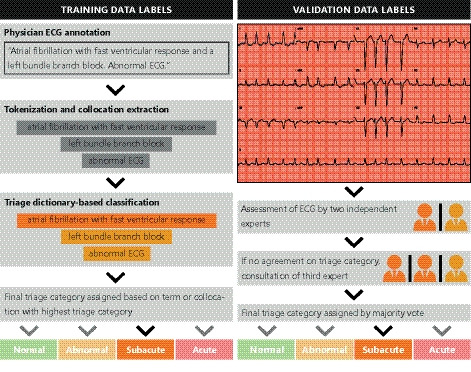
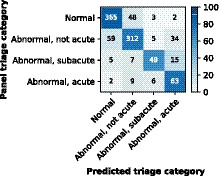
BACKGROUND The correct interpretation of the ECG is pivotal for the accurate diagnosis of many cardiac abnormalities, and conventional computerized interpretation has not been able to reach physician-level accuracy in detecting (acute) cardiac abnormalities. This study aims to develop and validate a deep neural network for comprehensive automated ECG triage in daily practice. METHODS AND RESULTS We developed a 37-layer convolutional residual deep neural network on a data set of free-text physician-annotated 12-lead ECGs. The deep neural network was trained on a data set with 336.835 recordings from 142.040 patients and validated on an independent validation data set (n=984), annotated by a panel of 5 cardiologists electrophysiologists. The 12-lead ECGs were acquired in all noncardiology departments of the University Medical Center Utrecht. The algorithm learned to classify these ECGs into the following 4 triage categories: normal, abnormal not acute, subacute, and acute. Discriminative performance is presented with overall and category-specific concordance statistics, polytomous discrimination indexes, sensitivities, specificities, and positive and negative predictive values. The patients in the validation data set had a mean age of 60.4 years and 54.3% were men. The deep neural network showed excellent overall discrimination with an overall concordance statistic of 0.93 (95% CI, 0.92-0.95) and a polytomous discriminatory index of 0.83 (95% CI, 0.79-0.87). CONCLUSIONS This study demonstrates that an end-to-end deep neural network can be accurately trained on unstructured free-text physician annotations and used to consistently triage 12-lead ECGs. When further fine-tuned with other clinical outcomes and externally validated in clinical practice, the demonstrated deep learning-based ECG interpretation can potentially improve time to treatment and decrease healthcare burden.
Keywords: deep learning; deep neural networks; electrocardiography; triage.
Figures
References
-
- Holst H, Ohlsson M, Peterson C, Edenbrandt L. A confident decision support system for interpreting electrocardiograms. Clin Physiol. 1999;19:410–418. - PubMed
-
- Diercks DB, Kontos MC, Chen AY, Pollack CV, Wiviott SD, Rumsfeld JS, Magid DJ, Gibler WB, Cannon CP, Peterson ED, et al. Utilization and impact of pre‐hospital electrocardiograms for patients with acute ST‐segment elevation myocardial infarction. J Am Coll Cardiol. 2009;53:161–166. - PubMed
-
- Eslava D, Dhillon S, Berger J, Homel P, Bergmann S. Interpretation of electrocardiograms by first‐year residents: the need for change. J Electrocardiol. 2009;42:693–697. - PubMed
-
- Salerno SM, Alguire PC, Waxman HS. Competency in interpretation of 12‐lead electrocardiograms: a summary and appraisal of published evidence. Ann Intern Med. 2003;138:751. - PubMed
-
- Schläpfer J, Wellens HJ. Computer‐interpreted electrocardiograms. J Am Coll Cardiol. 2017;70:1183–1192. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
