

Infection-related hospitalization after intensive immunosuppressive therapy among lupus nephritis and ANCA glomerulonephritis patients
- PMID: 32406300
- PMCID: PMC7269069
- DOI: 10.1080/0886022X.2020.1763400
Infection-related hospitalization after intensive immunosuppressive therapy among lupus nephritis and ANCA glomerulonephritis patients
Abstract
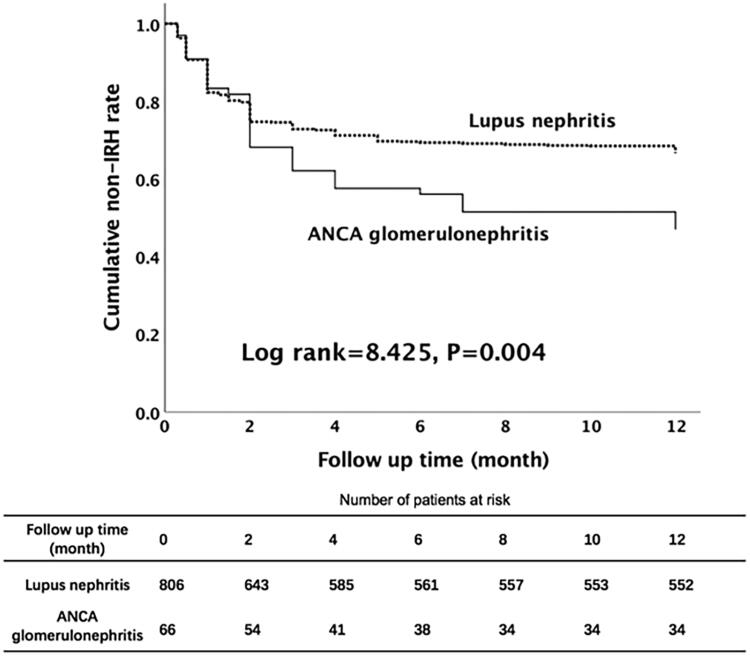
Introduction: This study aimed to investigate the clinical characteristics, risk factors, and outcomes of infection-related hospitalization (IRH) in patients with lupus nephritis (LN) and ANCA glomerulonephritis after intensive immunosuppressive therapy.Methods: Patients diagnosed with LN or ANCA glomerulonephritis who received intensive immunosuppressive therapy at the First Affiliated Hospital of Sun Yat-sen University from 2005 to 2014 were enrolled. Demographics, laboratory parameters, immunosuppressive agents, and IRH details were collected. Multivariable Cox regression was used, and hazard ratios (HRs) and 95% confidence intervals (CIs) were reported.Results: Totally, 872 patients with 806 LN and 66 ANCA glomerulonephritis were enrolled, and 304 (34.9%) patients with 433 episodes of IRH were recorded. ANCA glomerulonephritis patients were more vulnerable to IRH than LN patients (53.0% vs. 33.4%, p = .001). Multivariable Cox regression analysis showed that ANCA glomerulonephritis (HR = 1.62, 95% CI: 1.06-2.49, p = .027), diabetes (HR = 1.82, 95% CI: 1.03-3.22, p = .039) and a higher initial dose of prednisone (HR = 1.01, 95% CI: 1.00-1.02, p = .013) were associated with a higher likelihood of IRH. Higher albumin (HR = 0.96, 95% CI: 0.94-0.98, p < .001), globulin (HR = 0.98, 95% CI: 0.96-0.99, p = .008), and eGFR (HR = 0.99, 95% CI: 0.99-1.00, p < .001), were associated with a lower likelihood of IRH. The rates of transfer to ICU and mortality for ANCA glomerulonephritis patients were higher than those for LN patients (22.9% vs. 1.9%, p < .001, and 20.0% vs. 0.7%, p < .001, respectively).Conclusions: ANCA glomerulonephritis patients had a higher risk of IRH and poorer outcome once infected after intensive immunosuppressive therapy than LN patients. More strict control for infection risks is required for ANCA glomerulonephritis patients who undergo intensive immunosuppressive therapy.
Keywords: ANCA glomerulonephritis; Lupus nephritis; hospitalization; immunosuppression; infection.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
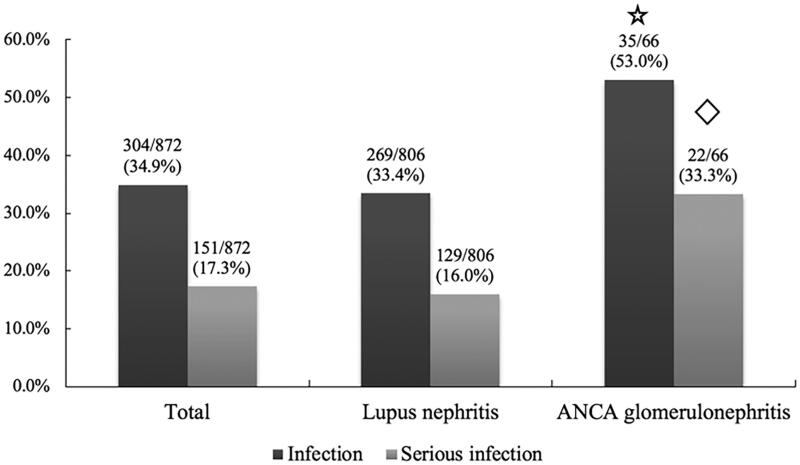
 p=.001 compared to lupus nephritis;
p=.001 compared to lupus nephritis;  p<.001 compared to lupus nephritis.
p<.001 compared to lupus nephritis.
Similar articles
-
Clinicopathologic characteristics and outcomes of lupus nephritis with positive antineutrophil cytoplasmic antibody.Ren Fail. 2020 Nov;42(1):244-254. doi: 10.1080/0886022X.2020.1735416. Ren Fail. 2020. PMID: 32228220 Free PMC article.
-
Clinicopathologic Characteristics and Outcomes of Lupus Nephritis With Antineutrophil Cytoplasmic Antibody: A Retrospective Study.Medicine (Baltimore). 2016 Jan;95(4):e2580. doi: 10.1097/MD.0000000000002580. Medicine (Baltimore). 2016. PMID: 26825903 Free PMC article.
-
Serious infections among adult Medicaid beneficiaries with systemic lupus erythematosus and lupus nephritis.Arthritis Rheumatol. 2015 Jun;67(6):1577-85. doi: 10.1002/art.39070. Arthritis Rheumatol. 2015. PMID: 25772621 Free PMC article.
-
Prevalence and clinical significance of ANCA positivity in lupus nephritis: a case series of 116 patients and literature review.J Nephrol. 2023 May;36(4):1059-1070. doi: 10.1007/s40620-023-01574-3. Epub 2023 Mar 20. J Nephrol. 2023. PMID: 36940001 Review.
-
ANCA-associated glomerulonephritis and lupus nephritis following COVID-19 vaccination: a case report and literature review.Front Immunol. 2024 Jan 8;14:1298622. doi: 10.3389/fimmu.2023.1298622. eCollection 2023. Front Immunol. 2024. PMID: 38299140 Free PMC article. Review.
Cited by
-
In-hospital mortality and associated factors in patients with systemic lupus erythematosus: analysis over more than 11 years in a reference hospital center.Rheumatol Int. 2023 Dec;43(12):2221-2231. doi: 10.1007/s00296-023-05469-1. Epub 2023 Sep 30. Rheumatol Int. 2023. PMID: 37776497
-
Corticosteroids are the major contributors to the risk for serious infections in autoimmune disorders with severe renal involvement.Clin Rheumatol. 2021 Aug;40(8):3285-3297. doi: 10.1007/s10067-021-05646-2. Epub 2021 Feb 17. Clin Rheumatol. 2021. PMID: 33595739
References
-
- Suarez-Fueyo A, Bradley SJ, Klatzmann D, et al. . T cells and autoimmune kidney disease. Nat Rev Nephrol. 2017;13(6):329–343. - PubMed
-
- Devarapu SK, Lorenz G, Kulkarni OP, et al. . Cellular and molecular mechanisms of autoimmunity and lupus nephritis. Int Rev Cell Mol Biol. 2017;332:43–154. - PubMed
-
- Alarcon GS. Multiethnic lupus cohorts: what have they taught us? Reumatol Clin. 2011;7(1):3–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous