

Long-term virologic responses to antiretroviral therapy among HIV-positive patients entering adherence clubs in Khayelitsha, Cape Town, South Africa: a longitudinal analysis
- PMID: 32406983
- PMCID: PMC7224308
- DOI: 10.1002/jia2.25476
Long-term virologic responses to antiretroviral therapy among HIV-positive patients entering adherence clubs in Khayelitsha, Cape Town, South Africa: a longitudinal analysis
Abstract
Introduction: In South Africa, an estimated 4.6 million people were accessing antiretroviral therapy (ART) in 2018. As universal Test and Treat is implemented, these numbers will continue to increase. Given the need for lifelong care for millions of individuals, differentiated service delivery models for ART services such as adherence clubs (ACs) for stable patients are required. In this study, we describe long-term virologic outcomes of patients who have ever entered ACs in Khayelitsha, Cape Town.
Methods: We included adult patients enrolled in ACs in Khayelitsha between January 2011 and December 2016 with a recorded viral load (VL) before enrolment. Risk factors for an elevated VL (VL >1000 copies/mL) and confirmed virologic failure (two consecutive VLs >1000 copies/mL one year apart) were estimated using Cox proportional hazards models. VL completeness over time was assessed.
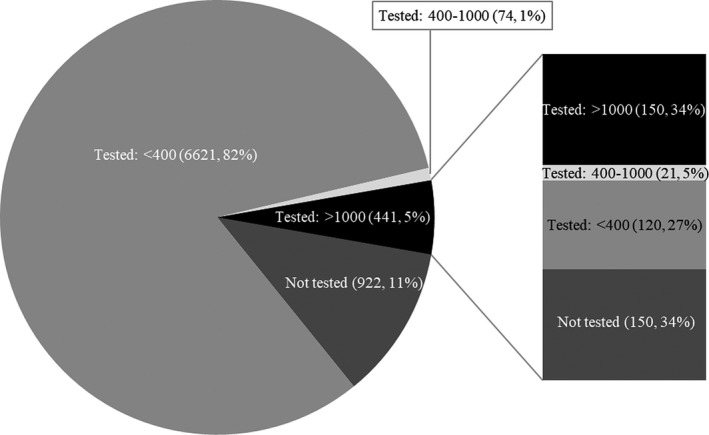
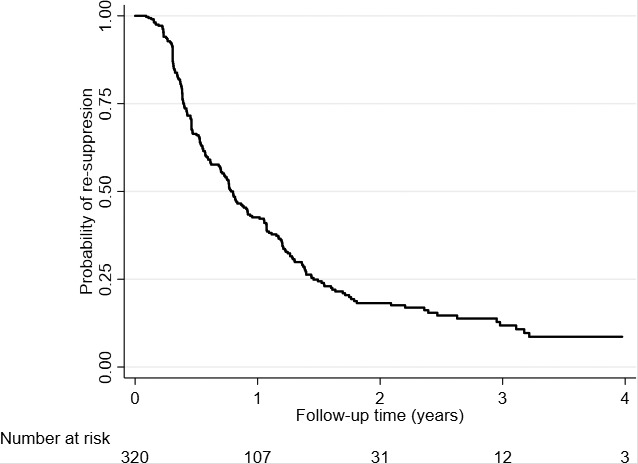
Results: Overall, 8058 patients were included in the analysis, contributing 16,047 person-years of follow-up from AC entry (median follow-up time 1.7 years, interquartile range [IQR]:0.9 to 2.9). At AC entry, 74% were female, 46% were aged between 35 and 44 years, and the median duration on ART was 4.8 years (IQR: 3.0 to 7.2). Among patients virologically suppressed at AC entry (n = 8058), 7136 (89%) had a subsequent VL test, of which 441 (6%) experienced an elevated VL (median time from AC entry 363 days, IQR: 170 to 728). Older age (adjusted hazard ratio [aHR] 0.64, 95% confidence interval [CI] 0.46 to 0.88), more recent year of AC entry (aHR 0.76, 95% CI 0.68 to 0.84) and higher CD4 count (aHR 0.67, 95% CI 0.54 to 0.84) were protective against experiencing an elevated VL. Among patients with an elevated VL, 52% (150/291) with a repeat VL test subsequently experienced confirmed virologic failure in a median time of 112 days (IQR: 56 to 168). Frequency of VL testing was constant over time (82 to 85%), with over 90% of patients remaining virologically suppressed.
Conclusions: This study demonstrates low prevalence of elevated VLs and confirmed virologic failure among patients who entered ACs. Although ACs were expanded rapidly, most patients were well monitored and remained stable, supporting the continued rollout of this model.
Keywords: HIV; Sub-Saharan Africa; adherence clubs; antiretroviral therapy; antiretroviral treatment; differentiated service delivery models; elevated viral load; viral load monitoring; virologic failure; virologic responses.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
Similar articles
-
High rates of retention and viral suppression in the scale-up of antiretroviral therapy adherence clubs in Cape Town, South Africa.J Int AIDS Soc. 2017 Jul 21;20(Suppl 4):21649. doi: 10.7448/IAS.20.5.21649. J Int AIDS Soc. 2017. PMID: 28770595 Free PMC article.
-
Virologic outcomes after early referral of stable HIV-positive adults initiating ART to community-based adherence clubs in Cape Town, South Africa: A randomised controlled trial.PLoS One. 2022 Nov 15;17(11):e0277018. doi: 10.1371/journal.pone.0277018. eCollection 2022. PLoS One. 2022. PMID: 36378660 Free PMC article. Clinical Trial.
-
Superior virologic and treatment outcomes when viral load is measured at 3 months compared to 6 months on antiretroviral therapy.J Int AIDS Soc. 2015 Sep 23;18(1):20092. doi: 10.7448/IAS.18.1.20092. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26403636 Free PMC article.
-
What do the implementation outcome variables tell us about the scaling-up of the antiretroviral treatment adherence clubs in South Africa? A document review.Health Res Policy Syst. 2019 Mar 14;17(1):28. doi: 10.1186/s12961-019-0428-z. Health Res Policy Syst. 2019. PMID: 30871565 Free PMC article. Review.
-
A meta-analysis of adherence to antiretroviral therapy and virologic responses in HIV-infected children, adolescents, and young adults.AIDS Behav. 2013 Jan;17(1):41-60. doi: 10.1007/s10461-012-0159-4. AIDS Behav. 2013. PMID: 22411426 Review.
Cited by
-
Health Worker Experiences of and Perspectives on Engaging Men in HIV Care: A Qualitative Study in Cape Town, South Africa.J Int Assoc Provid AIDS Care. 2020 Jan-Dec;19:2325958220935691. doi: 10.1177/2325958220935691. J Int Assoc Provid AIDS Care. 2020. PMID: 32597712 Free PMC article.
-
Brief Report: Time to Repeat Viral Load Testing Among Unsuppressed Adolescents and Young Adults Living With HIV in Kenya.J Acquir Immune Defic Syndr. 2020 Dec 15;85(5):606-611. doi: 10.1097/QAI.0000000000002498. J Acquir Immune Defic Syndr. 2020. PMID: 32897936 Free PMC article.
-
Uptake of community- versus clinic-based antiretroviral therapy dispensing in the Central Chronic Medication Dispensing and Distribution program in South Africa.J Int AIDS Soc. 2022 Jan;25(1):e25877. doi: 10.1002/jia2.25877. J Int AIDS Soc. 2022. PMID: 35077611 Free PMC article.
-
The viral load monitoring cascade in HIV treatment programmes in sub-Saharan Africa: a systematic review.BMC Public Health. 2024 Sep 27;24(1):2603. doi: 10.1186/s12889-024-20013-x. BMC Public Health. 2024. PMID: 39334013 Free PMC article.
-
Understanding Engagement in HIV Programmes: How Health Services Can Adapt to Ensure No One Is Left Behind.Curr HIV/AIDS Rep. 2020 Oct;17(5):458-466. doi: 10.1007/s11904-020-00522-1. Curr HIV/AIDS Rep. 2020. PMID: 32844274 Free PMC article. Review.
References
-
- UNAIDS . Fact Sheet ‐ Global AIDS update 2019 [Internet]. 2019. [cited 2019 Jul 16]. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_...
-
- The Western Cape Government . The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother‐to‐Child of HIV (PMTCT), Children, Adolescents and Adults [Internet]. Vol. 2016. 2016. [cited 2019 May 16]. Available from: https://www.westerncape.gov.za/assets/departments/health/wcgh233_hiv_pmt...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
