

Overall Survival of CDK4/6-Inhibitor-Based Treatments in Clinically Relevant Subgroups of Metastatic Breast Cancer: Systematic Review and Meta-Analysis
- PMID: 32407488
- PMCID: PMC7669227
- DOI: 10.1093/jnci/djaa071
Overall Survival of CDK4/6-Inhibitor-Based Treatments in Clinically Relevant Subgroups of Metastatic Breast Cancer: Systematic Review and Meta-Analysis
Abstract
Background: Cyclin-dependent kinases 4 and 6 (CDK4/6) inhibitors + endocrine therapy (ET) prolonged progression-free survival as first- or second-line therapy for hormone receptor-positive (HR+)/HER2-negative metastatic breast cancer prognosis. Given the recent publication of overall survival (OS) data for the 3 CDK4/6-inhibitors, we performed a meta-analysis to identify a more precise and reliable benefit from such treatments in specific clinical subgroups.
Methods: We conducted a systematic literature search to select all available phase II or III randomized clinical trials of CDK4/6-inhibitors + ET reporting OS data in first- or second-line therapy of HR+/HER2-negative pre- or postmenopausal metastatic breast cancer. A random effect model was applied for the analyses. Heterogeneity was assessed with I2statistic. Subgroup analysis was performed to explore the effect of study-level factors. The project was registered in the Open Science Framework database (doi: 10.17605/OSF.IO/TNZQP).
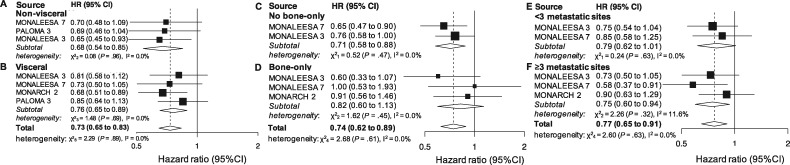
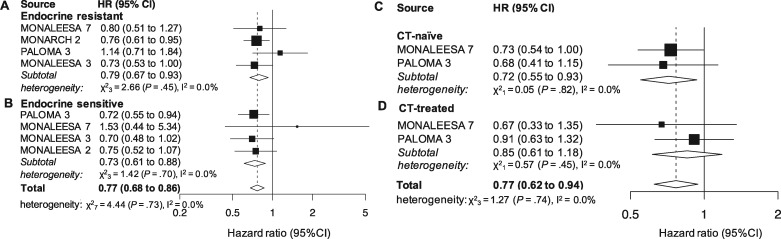
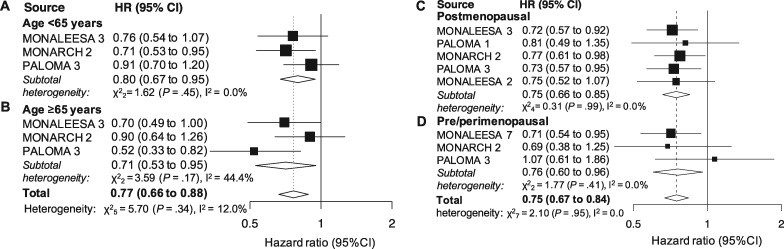
Results: Six studies were included in our analyses (3421 patients). A clear OS benefit was observed in patients without (hazard ratio [HR] = 0.68, 95% confidence interval [CI] = 0.54 to 0.85, I2 = 0.0%) and with visceral involvement (HR = 0.76, 95% CI = 0.65 to 0.89, I2 = 0.0%), with at least 3 metastatic sites (HR = 0.75, 95% CI = 0.60 to 0.94, I2 = 11.6%), in an endocrine-resistant (HR = 0.79, 95% CI = 0.67 to 0.93, I2 = 0.0%) and sensitive subset (HR = 0.73, 95% CI = 0.61 to 0.88, I2 = 0.0%), for younger than 65 years (HR = 0.80, 95% CI = 0.67 to 0.95, I2 = 0.0%) and 65 years or older (HR = 0.71, 95% CI = 0.53 to 0.95, I2 = 44.4%), in postmenopausal (HR = 0.76, 95% CI = 0.67 to 0.86, I2 = 0.0%) and pre- or perimenopausal setting (HR = 0.76, 95% CI = 0.60 to 0.96, I2 = 0.0%) as well as in chemotherapy-naïve patients (HR = 0.72, 95% CI = 0.55 to 0.93, I2 = 0.0%).
Conclusions: CDK4/6-inhibitors + ET combinations compared with ET alone improve OS independent of age, menopausal status, endocrine sensitiveness, and visceral involvement and should be preferred as upfront therapy instead of endocrine monotherapy.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Schettini F, Buono G, Cardalesi C, Desideri I, De Placido S, Del Mastro L. Hormone receptor/human epidermal growth factor receptor 2-positive breast cancer: where we are now and where we are going. Cancer Treat Rev. 2016;46:20–26. - PubMed
-
- Sledge GW, Toi M, Neven P, et al. MONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2- advanced breast cancer who had progressed while receiving endocrine therapy. J Clin Oncol. 2017;35(25):2875–2884. - PubMed
-
- Cristofanilli M, Turner NC, Bondarenko I, et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016;17(4):425–439. - PubMed
-
- Tripathy D, Im S-A, Colleoni M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. Lancet Oncol. 2018;19(7):904–915. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
