

Molecular Mechanisms of Premature Aging in Hemodialysis: The Complex Interplay Between Innate and Adaptive Immune Dysfunction
- PMID: 32408613
- PMCID: PMC7279398
- DOI: 10.3390/ijms21103422
Molecular Mechanisms of Premature Aging in Hemodialysis: The Complex Interplay Between Innate and Adaptive Immune Dysfunction
Abstract
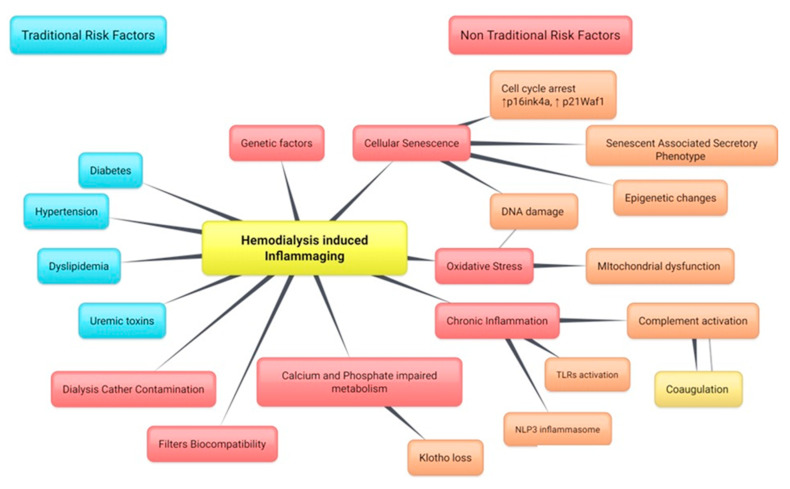
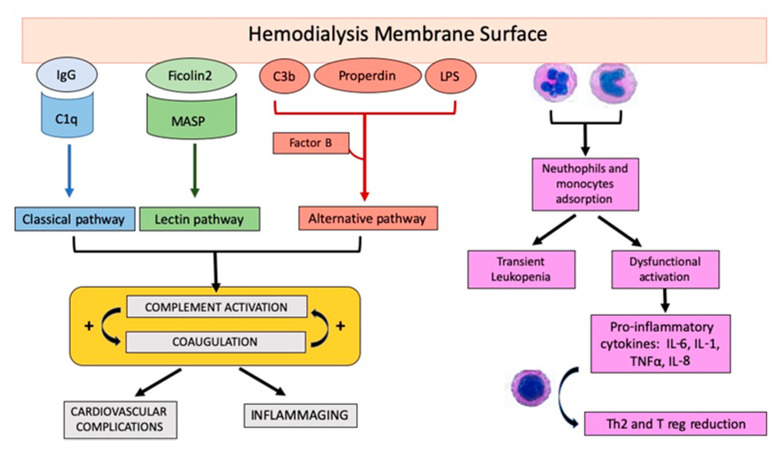
Hemodialysis (HD) patient are known to be susceptible to a wide range of early and long-term complication such as chronic inflammation, infections, malnutrition, and cardiovascular disease that significantly affect the incidence of mortality. A large gap between the number of people with end-stage kidney disease (ESKD) and patients who received kidney transplantation has been identified. Therefore, there is a huge need to explore the underlying pathophysiology of HD complications in order to provide treatment guidelines. The immunological dysregulation, involving both the innate and adaptive response, plays a crucial role during the HD sessions and in chronic, maintenance treatments. Innate immune system mediators include the dysfunction of neutrophils, monocytes, and natural killer (NK) cells with signaling mediated by NOD-like receptor P3 (NLRP3) and Toll-like receptor 4 (TLR4); in addition, there is a significant activation of the complement system that is mediated by dialysis membrane-surfaces. These effectors induce a persistent, systemic, pro-inflammatory, and pro-coagulant milieu that has been described as inflammaging. The adaptive response, the imbalance in the CD4+/CD8+ T cell ratio, and the reduction of Th2 and regulatory T cells, together with an altered interaction with B lymphocyte by CD40/CD40L, have been mainly implicated in immune system dysfunction. Altogether, these observations suggest that intervention targeting the immune system in HD patients could improve morbidity and mortality. The purpose of this review is to expand our understanding on the role of immune dysfunction in both innate and adaptive response in patients undergoing hemodialysis treatment.
Keywords: complement; hemodialysis; kidney; premature aging.
Conflict of interest statement
G.C. received Conference Grant by Estor SPA [Italy].
Figures
References
-
- Recio-Mayoral A., Banerjee D., Streather C., CarlosKaski J. Endothelial dysfunction, inflammation and atherosclerosis in chronic kidney disease—A cross-sectional study of predialysis, dialysis and kidney-transplantation patients. Atherosclerosis. 2011;216:446–451. doi: 10.1016/j.atherosclerosis.2011.02.017. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
