

Machine learning-based risk model using 123I-metaiodobenzylguanidine to differentially predict modes of cardiac death in heart failure
- PMID: 32410060
- PMCID: PMC8873155
- DOI: 10.1007/s12350-020-02173-6
Machine learning-based risk model using 123I-metaiodobenzylguanidine to differentially predict modes of cardiac death in heart failure
Abstract
Background: Cardiac sympathetic dysfunction is closely associated with cardiac mortality in patients with chronic heart failure (CHF). We analyzed the ability of machine learning incorporating 123I-metaiodobenzylguanidine (MIBG) to differentially predict risk of life-threatening arrhythmic events (ArE) and heart failure death (HFD).
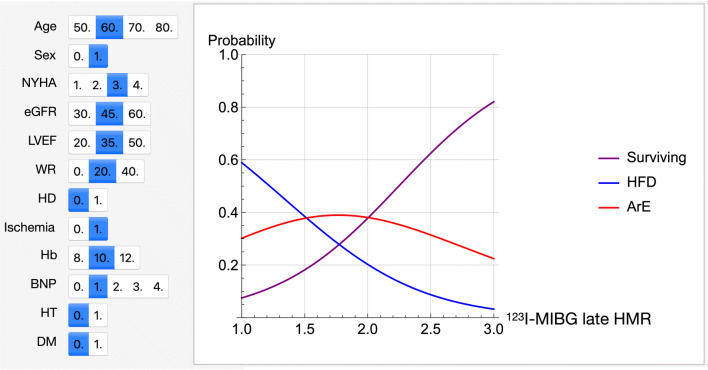
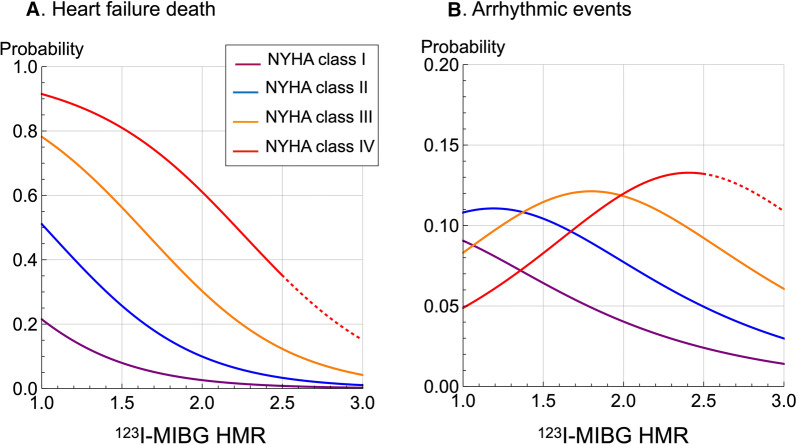
Methods and results: A model was created based on patients with documented 2-year outcomes of CHF (n = 526; age, 66 ± 14 years). Classifiers were trained using 13 variables including age, gender, NYHA functional class, left ventricular ejection fraction and planar 123I-MIBG heart-to-mediastinum ratio (HMR). ArE comprised arrhythmic death and appropriate therapy with an implantable cardioverter defibrillator. The probability of ArE and HFD at 2 years was separately calculated based on appropriate classifiers. The probability of HFD significantly increased as HMR decreased when any variables were combined. However, the probability of arrhythmic events was maximal when HMR was intermediate (1.5-2.0 for patients with NYHA class III). Actual rates of ArE were 3% (10/379) and 18% (27/147) in patients at low- (≤ 11%) and high- (> 11%) risk of developing ArE (P < .0001), respectively, whereas those of HFD were 2% (6/328) and 49% (98/198) in patients at low-(≤ 15%) and high-(> 15%) risk of HFD (P < .0001).
Conclusion: A risk model based on machine learning using clinical variables and 123I-MIBG differentially predicted ArE and HFD as causes of cardiac death.
Keywords: Risk stratification; arrhythmia; artificial intelligence; cardiac mortality; neuroimaging.
© 2020. The Author(s).
Figures





References
-
- Agostini D, Verberne HJ, Burchert W, Knuuti J, Povinec P, Sambuceti G, et al. I-123-mIBG myocardial imaging for assessment of risk for a major cardiac event in heart failure patients: Insights from a retrospective European multicenter study. Eur J Nucl Med Mol Imaging. 2008;35:535–546. doi: 10.1007/s00259-007-0639-3. - DOI - PubMed
-
- Verschure DO, Veltman CE, Manrique A, Somsen GA, Koutelou M, Katsikis A, et al. For what endpoint does myocardial 123I-MIBG scintigraphy have the greatest prognostic value in patients with chronic heart failure? Results of a pooled individual patient data meta-analysis. Eur Heart J Cardiovasc Imaging. 2014;15:996–1003. doi: 10.1093/ehjci/jeu044. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
