

Pathophysiology of Chronic Inflammatory Demyelinating Polyneuropathy: Insights into Classification and Therapeutic Strategy
- PMID: 32410146
- PMCID: PMC7606443
- DOI: 10.1007/s40120-020-00190-8
Pathophysiology of Chronic Inflammatory Demyelinating Polyneuropathy: Insights into Classification and Therapeutic Strategy
Abstract
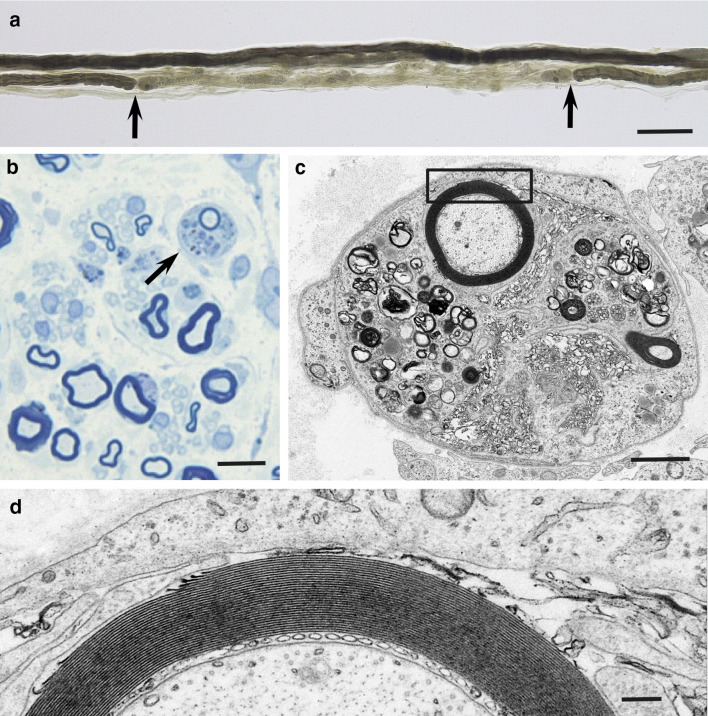
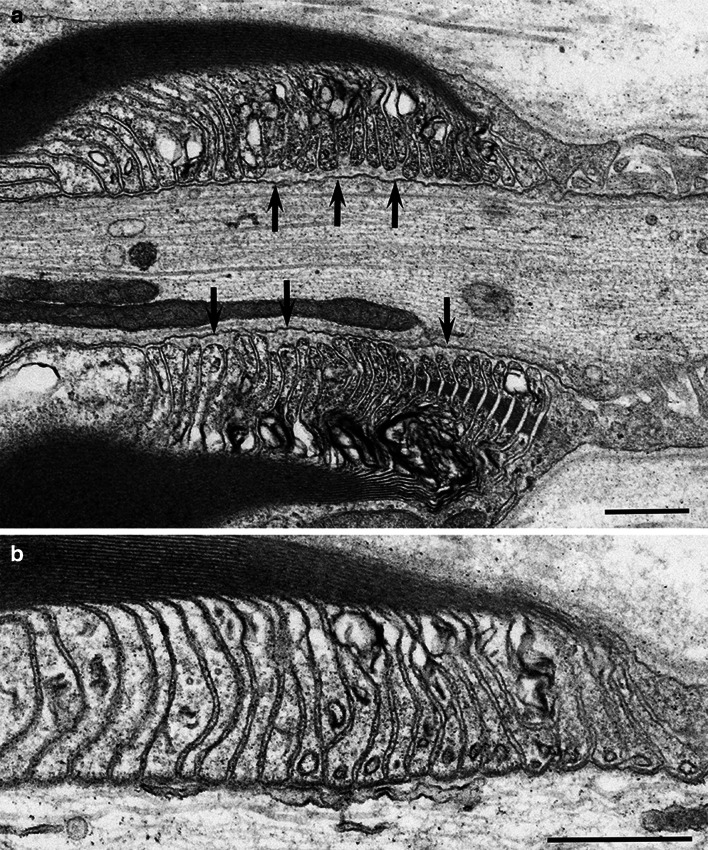
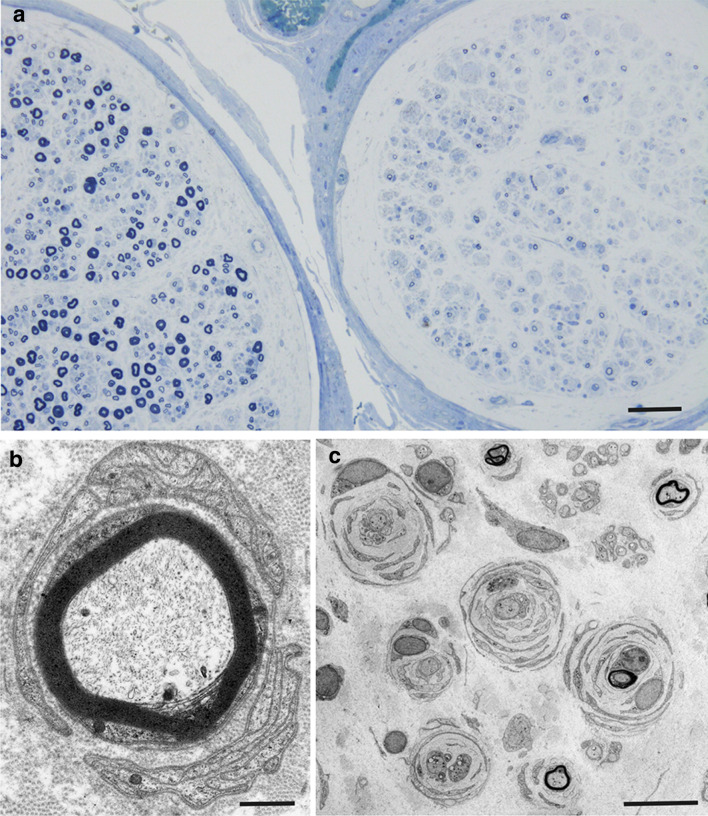
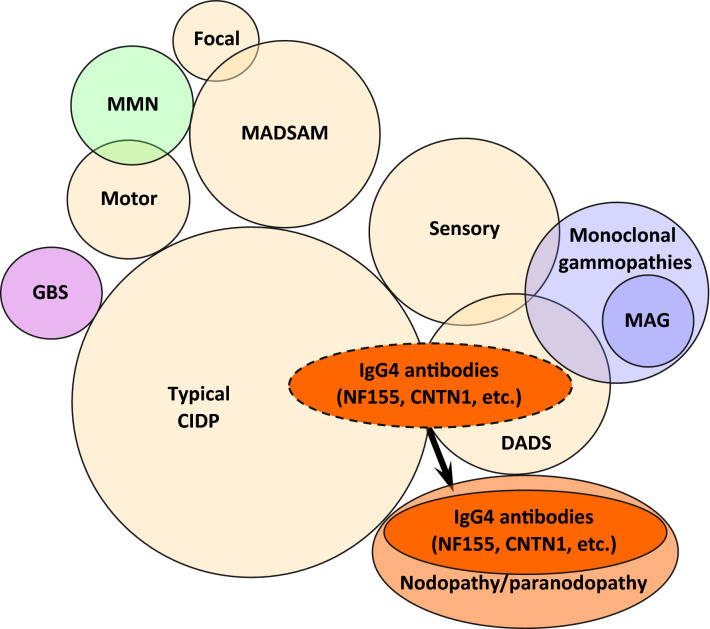
Chronic inflammatory demyelinating polyneuropathy (CIDP) is classically defined as polyneuropathy with symmetric involvement of the proximal and distal portions of the limbs. In addition to this "typical CIDP", the currently prevailing diagnostic criteria proposed by the European Federation of Neurological Societies and Peripheral Nerve Society (EFNS/PNS) define "atypical CIDP" as encompassing the multifocal acquired demyelinating sensory and motor (MADSAM), distal acquired demyelinating symmetric (DADS), pure sensory, pure motor, and focal subtypes. Although macrophage-induced demyelination is considered pivotal to the pathogenesis of CIDP, recent studies have indicated the presence of distinctive mechanisms initiated by autoantibodies against paranodal junction proteins, such as neurofascin 155 and contactin 1. These findings led to the emergence of the concept of nodopathy or paranodopathy. Patients with these antibodies tend to show clinical features compatible with typical CIDP or DADS, particularly the latter. In contrast, classical macrophage-induced demyelination is commonly found in some patients in each major subtype, including the typical CIDP, DADS, MADSAM, and pure sensory subtypes. Differences in the distribution of lesions and the repair processes underlying demyelination by Schwann cells may determine the differences among subtypes. In particular, the preferential involvement of proximal and distal nerve segments has been suggested to occur in typical CIDP, whereas the involvement of the middle nerve segments is conspicuous in MADSAM. These findings suggest that humoral rather than cellular immunity predominates in the former because nerve roots and neuromuscular junctions lack blood-nerve barriers. Treatment for CIDP consists of intravenous immunoglobulin (IVIg) therapy, steroids, and plasma exchange, either alone or in combination. However, patients with anti-neurofascin 155 and contactin 1 antibodies are refractory to IVIg. It has been suggested that rituximab, a monoclonal antibody to CD20, could have efficacy in these patients. Further studies are needed to validate the CIDP subtypes defined by the EFNS/PNS from the viewpoint of pathogenesis and establish therapeutic strategies based on the pathophysiologies specific to each subtype.
Keywords: Demyelination; Electron microscopy; Macrophage; Node of Ranvier; Paranode; Pathogenesis; Pathology; Schwann cell; Treatment; Ultrastructure.
Conflict of interest statement
Haruki Koike and Masahisa Katsuno have nothing to disclose.
Figures
References
-
- Dyck PJ, Lais AC, Ohta M, Bastron JA, Okazaki H, Groover RV. Chronic inflammatory polyradiculoneuropathy. Mayo Clin Proc. 1975;50:621–637. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
