

Prognostic impact of nutritional status and physical capacity in elderly patients with acute decompensated heart failure
- PMID: 32410337
- PMCID: PMC7373881
- DOI: 10.1002/ehf2.12743
Prognostic impact of nutritional status and physical capacity in elderly patients with acute decompensated heart failure
Abstract
Aims: Nutritional status as well as physical capacity is related to prognosis in patients with heart failure. The purpose of this study was to explore a simple prognostic indicator in patients with acute decompensated heart failure (ADHF) by including both nutritional status and physical capacity.
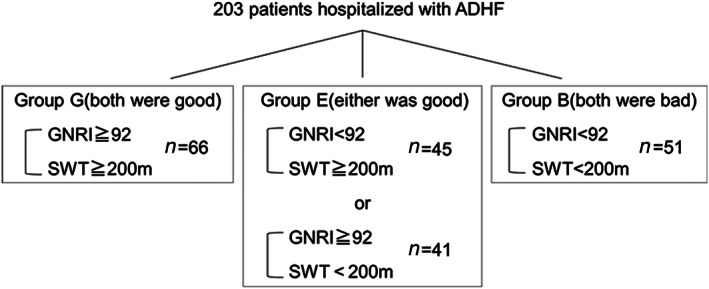
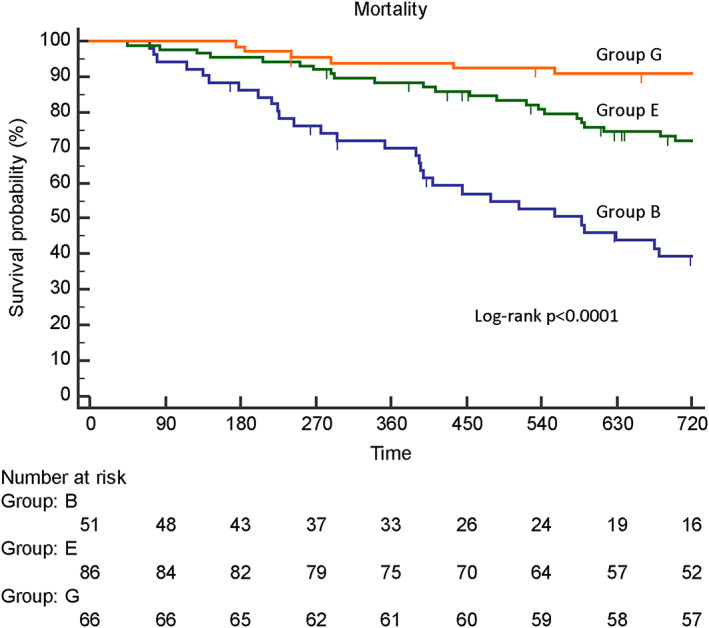
Methods and results: Patients hospitalized with ADHF (N = 203; mean age, 81 years) were enrolled. We evaluated the geriatric nutritional risk index (GNRI) on hospital admission and at discharge. A GNRI score < 92 was defined as malnutrition. Physical capacity was evaluated by simple walking test to determine if patients could walk 200 m, with a Borg scale score ≤ 13, without critical changes in vital signs. Primary endpoints were mortality and heart failure rehospitalization within 2 years. A total of 49% and 48% of patients showed malnutrition on admission and at discharge, respectively. Malnutrition at discharge was more strongly related to mortality [hazard ratio (HR) 3.382, 95% confidence interval (CI) 1.900-6.020, P < 0.0001)] than that on admission (HR 2.448, 95% CI 1.442-4.157, P = 0.001) by univariable analysis. Malnutrition at discharge was related to mortality (HR 2.370, 95% CI 1.166-4.814, P = 0.02), but malnutrition on admission was not related (HR 1.538, 95% CI 0.823-2.875, P = 0.18) by multivariable analysis. Almost half of patients (45%) could not walk 200 m, which was significantly related to mortality by univariable analysis (HR 3.303, 95% CI 1.905-5.727, P < 0.0001), but was not by multivariable analysis (HR 1.990, 95% CI 0.999-3.962, P = 0.05). The combined index including both GNRI and simple walking test was an independent and stronger predictor of mortality than either index alone by multivariable analysis (HR 2.249, 95% CI 1.362-3.716, P < 0.01). Neither malnutrition nor low physical capacity was related to heart failure rehospitalization by univariable analysis (HR 0.702, 95% CI 0.483-1.020, P = 0.06; HR 1.047, 95% CI 0.724-1.515, P = 0.81, respectively). Malnutrition at discharge significantly reduced heart failure rehospitalization by multivariable analysis (HR 0.431, 95% CI 0.266-0.698, P < 0.01). When patients were classified into Group G (both nutritional status and physical capacity at discharge were good), Group E (either was good), and Group B (both were bad), mortality rates were significantly different among the groups (log rank P < 0.0001).
Conclusion: A simple indicator including both nutritional status and physical capacity may predict 2 year mortality in elderly patients with ADHF.
Keywords: Acute decompensated heart failure; Elderly patients; Geriatric nutritional risk index; Simple walking test.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
Haruhiko Abe has received grants from Nippon Boehringer Ingelheim. Yasunori Ueda has received grants from Nihon Kohden. Masaaki Uematsu has received grants from Nippon Boehringer Ingelheim, Daiichi Sankyo Co Ltd. Yukihiro Koretsune has received remuneration from Daiichi Sankyo Co Ltd. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Sze S, Zhang J, Pellicori P, Morgan D, Hoye A, Clark AL. Prognostic value of simple frailty and malnutrition screening tools in patients with acute heart failure due to left ventricular systolic dysfunction. Clin Res Cardiol 2017; 106: 533–541. - PubMed
-
- Narumi T, Arimoto T, Funayama A, Kadowaki S, Otaki Y, Nishiyama S, Takahashi H, Shishido T, Miyashita T, Miyamoto T, Watanabe T, Kubota I. Prognostic importance of objective nutritional indexes in patients with chronic heart failure. J Cardiol 2013; 62: 307–313. - PubMed
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA. Frailty in older adults: evidence for a phenotype; Cardiovascular Health Study Collaborative Research Group. Journals of gerontology Ser A Biol Sci Med Sci 2001; 56: M146–156. - PubMed
-
- Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, Chou MY, Chen LY, Hsu PS, Krairit O, Lee JS, Lee WJ, Lee Y, Liang CK, Limpawattana P, Lin CS, Peng LN, Satake S, Suzuki T, Won CW, Wu CH, Wu SN, Zhang T, Zeng P, Akishita M, Arai H. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014; 15: 95–101. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
