

Incidence, Microbiology, and Outcomes in Patients Hospitalized With Infective Endocarditis
- PMID: 32410460
- PMCID: PMC7306256
- DOI: 10.1161/CIRCULATIONAHA.119.044913
Incidence, Microbiology, and Outcomes in Patients Hospitalized With Infective Endocarditis
Erratum in
-
Correction to: Incidence, Microbiology, and Outcomes in Patients Hospitalized With Infective Endocarditits.Circulation. 2020 Jun 23;141(25):e960. doi: 10.1161/CIR.0000000000000879. Epub 2020 Jun 22. Circulation. 2020. PMID: 32568584 Free PMC article. No abstract available.
Abstract
Background: Despite improvements in management, infective endocarditis remains associated with high mortality and morbidity. We describe temporal changes in the incidence, microbiology, and outcomes of infective endocarditis and the effect of changes in national antibiotic prophylaxis guidelines on incident infective endocarditis.
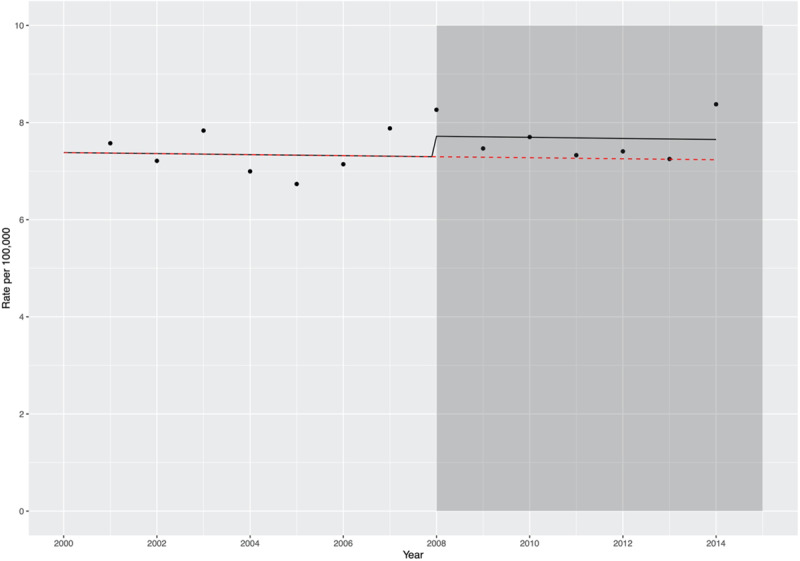
Methods: Using a Scotland-wide, individual-level linkage approach, all patients hospitalized with infective endocarditis from 1990 to 2014 were identified and linked to national microbiology, prescribing, and morbidity and mortality datasets. Linked data were used to evaluate trends in the crude and age- and sex-adjusted incidence and outcomes of infective endocarditis hospitalizations. From 2008, microbiology data and associated outcomes adjusted for patient demographics and comorbidity were also analyzed. An interrupted time series analysis was performed to evaluate incidence before and after changes to national antibiotic prophylaxis guidelines.
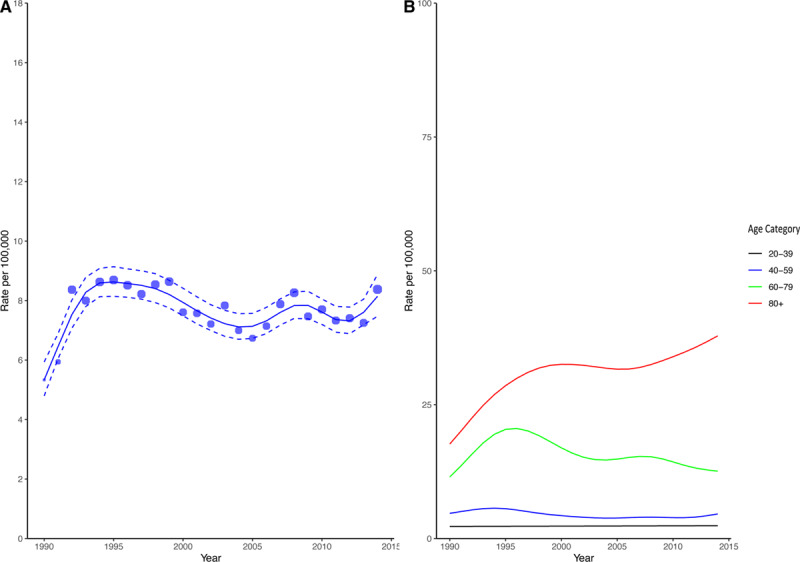
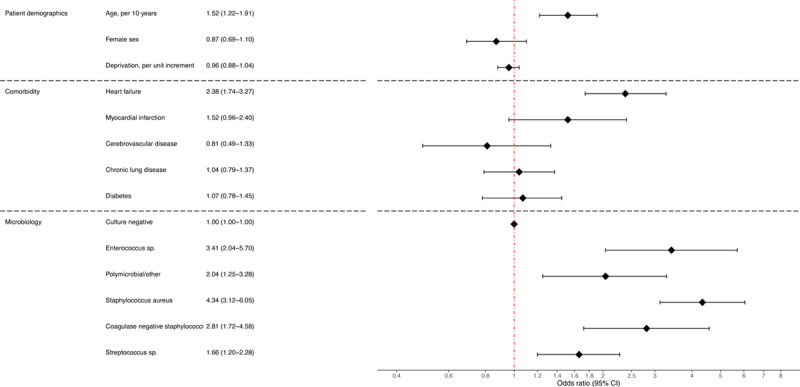
Results: There were 7638 hospitalizations (65±17 years, 51% females) with infective endocarditis. The estimated crude hospitalization rate increased from 5.3/100 000 (95% CI, 4.8-5.9) to 8.6/100 000 (95% CI, 8.1-9.1) between 1990 and 1995 but remained stable thereafter. There was no change in crude incidence following the 2008 change in antibiotic prophylaxis guidelines (relative risk of change 1.06 [95% CI, 0.94-1.20]). The incidence rate in patients >80 years of age doubled from 1990 to 2014 (17.7/100 000 [95% CI, 13.4-23.3] to 37.9/100 000 [95% CI, 31.5-45.5]). The predicted 1-year age- and comorbidity-adjusted case fatality rate for a 65-year-old patient decreased in women (27.3% [95% CI, 24.6-30.2] to 23.7% [95% CI, 21.1-26.6]) and men (30.7% [95% CI, 27.7-33.8] to 26.8% [95% CI, 24.0-29.7]) from 1990 to 2014. Blood culture data were available from 2008 (n=2267/7638, 30%), with positive blood cultures recorded in 42% (950/2267). Staphylococcus (403/950, 42.4%) and streptococcus (337/950, 35.5%) species were most common. Staphylococcus aureus and enterococcus had the highest 1-year mortality (adjusted odds ratio 4.34 [95% CI, 3.12-6.05] and 3.41 [95% CI, 2.04-5.70], respectively).
Conclusions: Despite changes in antibiotic prophylaxis guidelines, the crude incidence of infective endocarditis has remained stable. However, the incidence rate has doubled in the elderly. Positive blood cultures were observed in less than half of patients, with Staphylococcus aureus and enterococcus bacteremia associated with worse outcomes.
Keywords: antibiotic; antibiotic prophylaxis; incidence; infective endocarditis; mortality; outcomes.
Figures
References
-
- Thuny F, Grisoli D, Collart F, Habib G, Raoult D. Management of infective endocarditis: challenges and perspectives. Lancet. 2012;379:965–975. doi: 10.1016/S0140-6736(11)60755-1. - PubMed
-
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Dulgheru R, El Khoury G, Erba PA, Iung B, et al. ESC Scientific Document Group. 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36:3075–3128. doi: 10.1093/eurheartj/ehv319. - PubMed
-
- Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, Bolger A, Cabell CH, Takahashi M, Baltimore RS, et al. American Heart Association. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2008;139 Suppl:3S–24S. doi: 10.14219/jada.archive.2008.0346. - PubMed
