

Development and validation of a hypoxia-immune-based microenvironment gene signature for risk stratification in gastric cancer
- PMID: 32410620
- PMCID: PMC7226948
- DOI: 10.1186/s12967-020-02366-0
Development and validation of a hypoxia-immune-based microenvironment gene signature for risk stratification in gastric cancer
Abstract
Background: Increasing evidences have found that the clinical importance of the interaction between hypoxia and immune status in gastric cancer microenvironment. However, reliable prognostic signatures based on combination of hypoxia and immune status have not been well-established. This study aimed to develop a hypoxia-immune-based gene signature for risk stratification in gastric cancer.
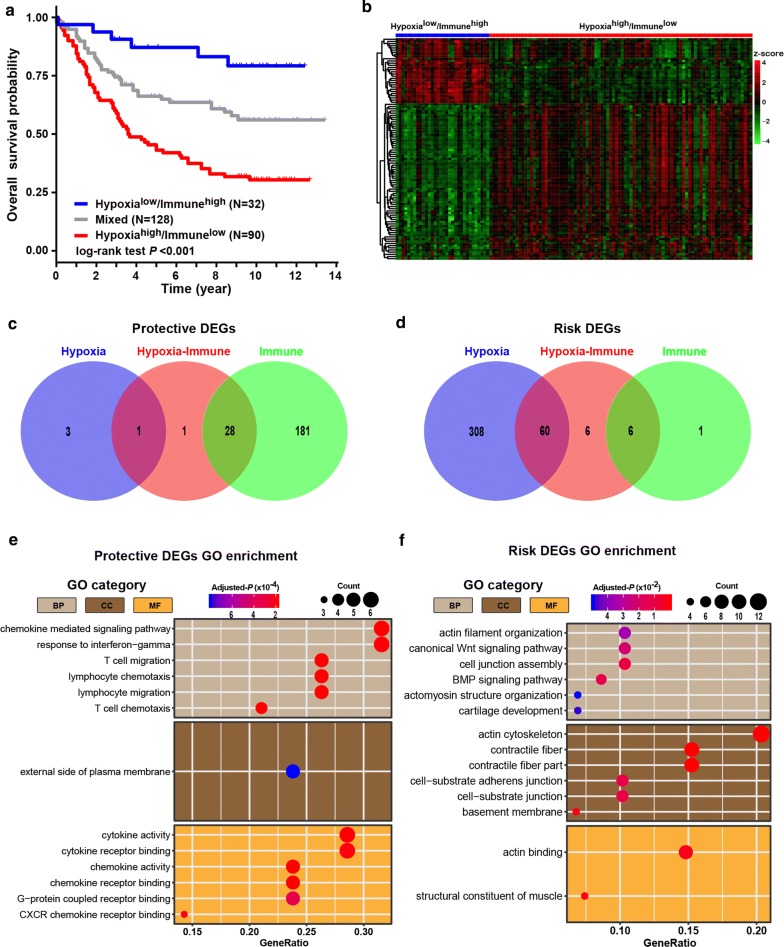
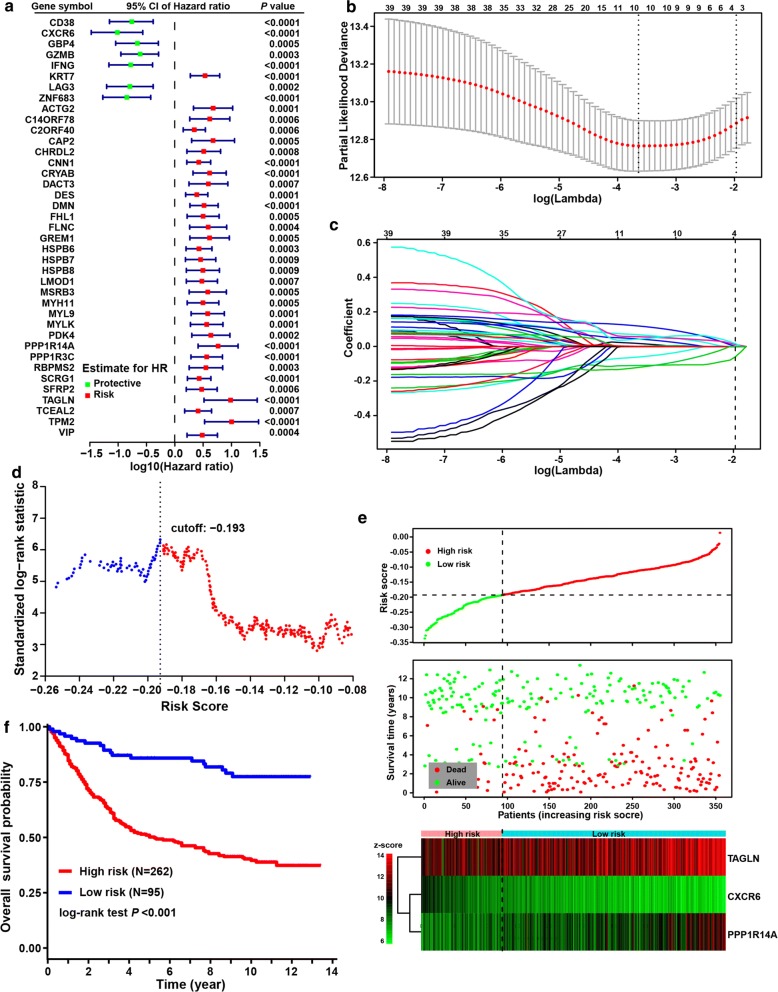
Methods: Hypoxia and immune status was estimated with transcriptomic profiles for a discovery cohort from GEO database using the t-SNE and ESTIMATE algorithms, respectively. The Cox regression model with the LASSO method was applied to identify prognostic genes and to develop a hypoxia-immune-based gene signature. The TCGA cohort and two independent cohorts from GEO database were used for external validation.
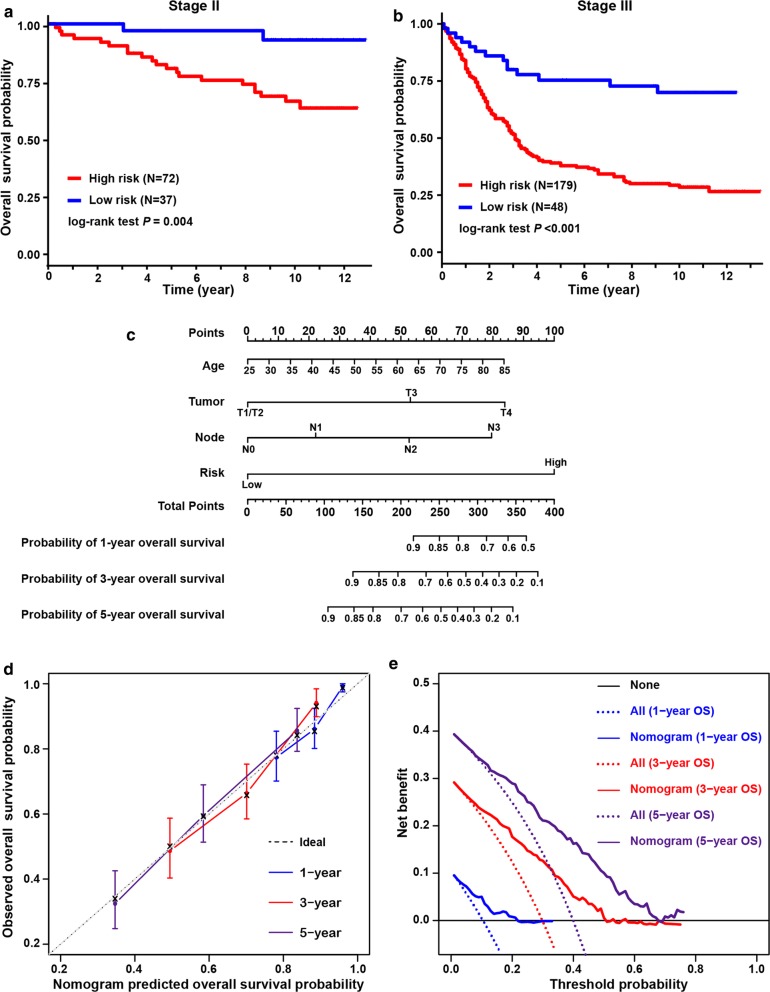
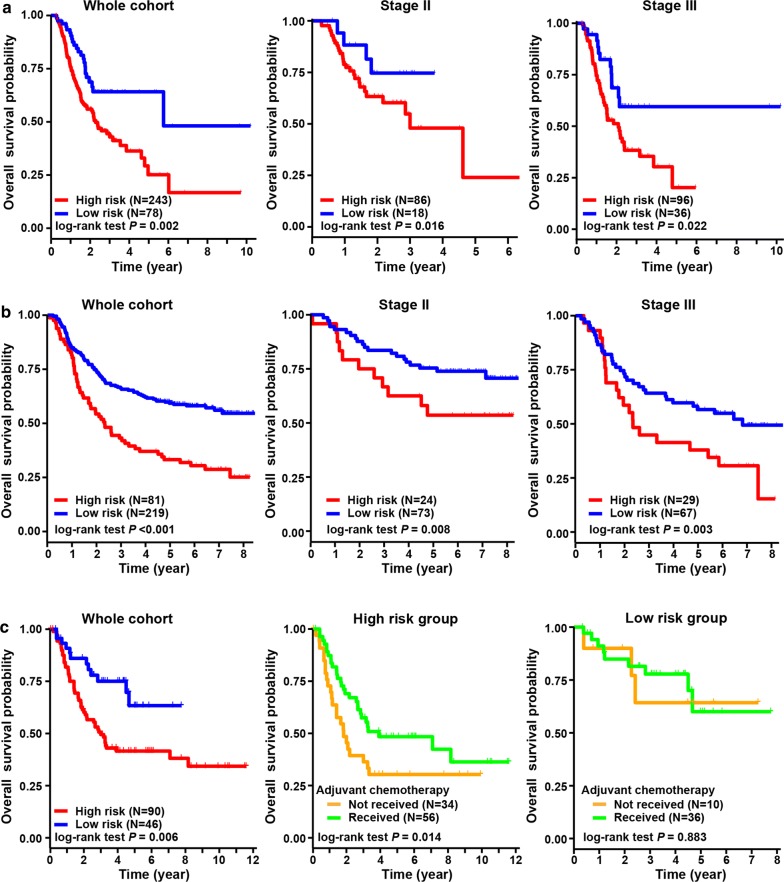
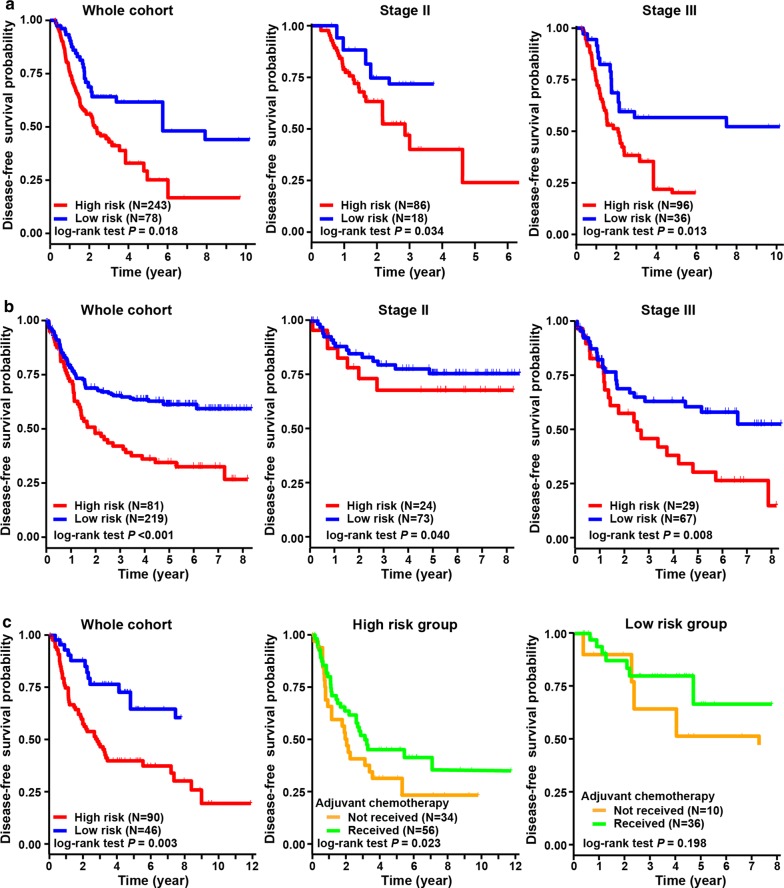
Results: Low hypoxia status (p < 0.001) and high immune status (p = 0.005) were identified as favorable factors for patients' overall survival. By using the LASSO model, four genes, including CXCR6, PPP1R14A and TAGLN, were identified to construct a gene signature for risk stratification. In the discovery cohort (n = 357), patients with low risk yielded better outcomes than those with high risk regarding overall survival across and within TNM stage subgroups. Multivariate analysis identified the hypoxia-immune-based gene signature as an independent prognostic factor (p < 0.001). A nomogram integrating the gene signature and known risk factors yielded better performance and net benefits in calibration and decision curve analyses. Similar results were validated in the TCGA (n = 321) and two independent GEO (n = 300 and n = 136, respectively) cohorts.
Conclusions: The hypoxia-immune-based gene signature represents a promising tool for risk stratification tool in gastric cancer. It might serve as a prognostic classifier for clinical decision-making regarding individualized prognostication and treatment, and follow-up scheduling.
Keywords: Gastric cancer; Hypoxia; Immune; Microenvironment; Prediction; Prognosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Ajani JA, D’Amico TA, Almhanna K, Bentrem DJ, Chao J, Das P, et al. Gastric cancer, Version 32016, NCCN Clinical Practice Guidelines In Oncology. JNCCN. 2016;14(10):1286–1312. - PubMed
-
- Shah MA, Ajani JA. Gastric cancer–an enigmatic and heterogeneous disease. JAMA. 2010;303(17):1753–1754. - PubMed
-
- Noh SH, Park SR, Yang HK, Chung HC, Chung IJ, Kim SW, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(12):1389–1396. - PubMed
-
- Hanahan D, Coussens LM. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. 2012;21(3):309–322. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
