

Augmented reality-based navigation increases precision of pedicle screw insertion
- PMID: 32410636
- PMCID: PMC7227090
- DOI: 10.1186/s13018-020-01690-x
Augmented reality-based navigation increases precision of pedicle screw insertion
Abstract
Background: Precise insertion of pedicle screws is important to avoid injury to closely adjacent neurovascular structures. The standard method for the insertion of pedicle screws is based on anatomical landmarks (free-hand technique). Head-mounted augmented reality (AR) devices can be used to guide instrumentation and implant placement in spinal surgery. This study evaluates the feasibility and precision of AR technology to improve precision of pedicle screw insertion compared to the current standard technique.
Methods: Two board-certified orthopedic surgeons specialized in spine surgery and two novice surgeons were each instructed to drill pilot holes for 40 pedicle screws in eighty lumbar vertebra sawbones models in an agar-based gel. One hundred and sixty pedicles were randomized into two groups: the standard free-hand technique (FH) and augmented reality technique (AR). A 3D model of the vertebral body was superimposed over the AR headset. Half of the pedicles were drilled using the FH method, and the other half using the AR method.
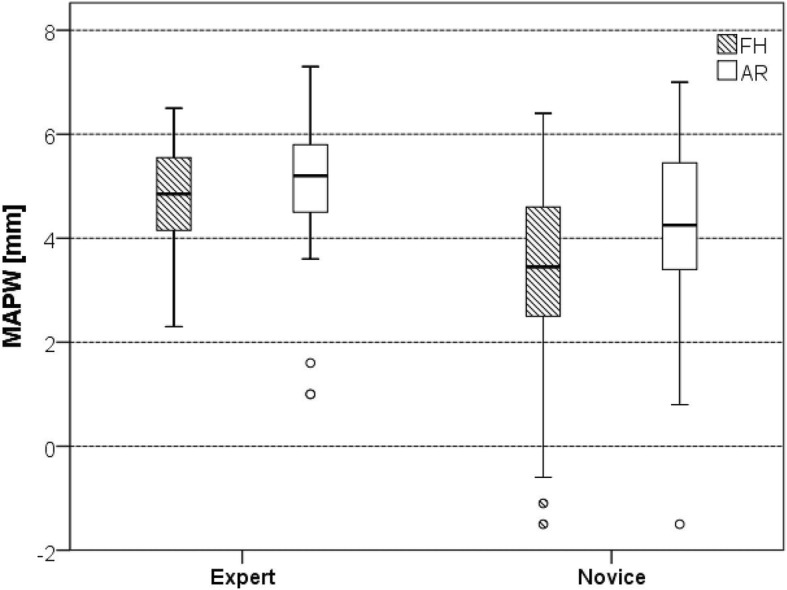
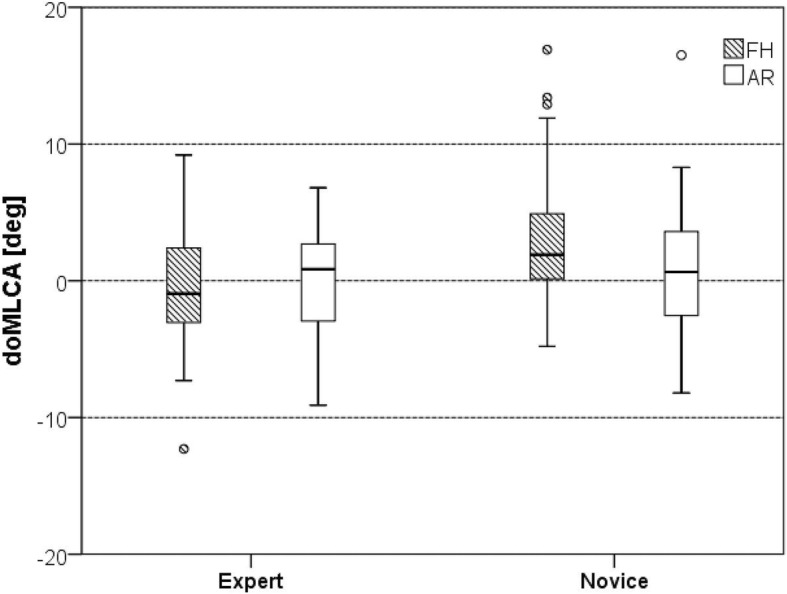
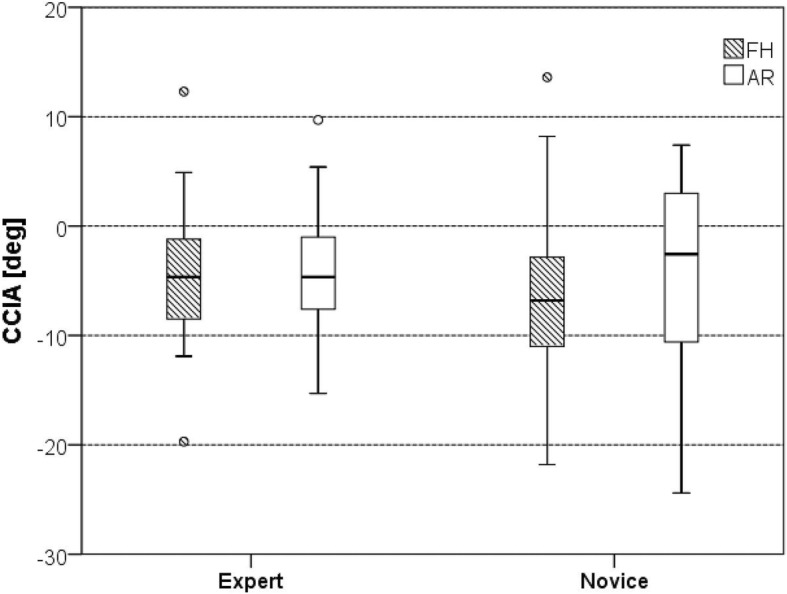
Results: The average minimal distance of the drill axis to the pedicle wall (MAPW) was similar in both groups for expert surgeons (FH 4.8 ± 1.0 mm vs. AR 5.0 ± 1.4 mm, p = 0.389) but for novice surgeons (FH 3.4 mm ± 1.8 mm, AR 4.2 ± 1.8 mm, p = 0.044). Expert surgeons showed 0 primary drill pedicle perforations (PDPP) in both the FH and AR groups. Novices showed 3 (7.5%) PDPP in the FH group and one perforation (2.5%) in the AR group, respectively (p > 0.005). Experts showed no statistically significant difference in average secondary screw pedicle perforations (SSPP) between the AR and the FH set 6-, 7-, and 8-mm screws (p > 0.05). Novices showed significant differences of SSPP between most groups: 6-mm screws, 18 (45%) vs. 7 (17.5%), p = 0.006; 7-mm screws, 20 (50%) vs. 10 (25%), p = 0.013; and 8-mm screws, 22 (55%) vs. 15 (37.5%), p = 0.053, in the FH and AR group, respectively. In novices, the average optimal medio-lateral convergent angle (oMLCA) was 3.23° (STD 4.90) and 0.62° (STD 4.56) for the FH and AR set screws (p = 0.017), respectively. Novices drilled with a higher precision with respect to the cranio-caudal inclination angle (CCIA) category (p = 0.04) with AR.
Conclusion: In this study, the additional anatomical information provided by the AR headset superimposed to real-world anatomy improved the precision of drilling pilot holes for pedicle screws in a laboratory setting and decreases the effect of surgeon's experience. Further technical development and validations studies are currently being performed to investigate potential clinical benefits of the herein described AR-based navigation approach.
Conflict of interest statement
See submitted statements of conflict of interest. One author, MF, states that he is the founder of a company developing AR-based navigation method. This involvement, however, is not a direct conflict of interest. The other authors declare that they have no competing interests.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
