An official website of the United States government
The .gov means it’s official.
Federal government websites often end in .gov or .mil. Before
sharing sensitive information, make sure you’re on a federal
government site.
The site is secure.
The https:// ensures that you are connecting to the
official website and that any information you provide is encrypted
and transmitted securely.
Dural arteriovenous fistula (dAVF) accounts for approximately 10% of all intracranial vascular malformations. While they can be benign lesions, the presence of retrograde venous drainage and cortical venous reflux makes the natural course of these lesions aggressive high risk of haemorrhage, neurological injury and mortality. Endovascular treatment is often the first line of treatment for dAVF. Both transarterial and transvenous approaches are used to cure dAVF. The selection of treatment approach depends on the angioarchitecture of the dAVF, the location, the direction of venous flow. Surgery and, to a lesser extent, stereotactic radiosurgery are used when endovascular approaches are impossible or unsuccessful.
Competing interests: GPC is a consultant for Medtronic, Stryker and MicroVention. ALC is a consultant for Medtronic, Stryker, MicroVention and InNeuroCo.
Figures
Figure 1
Transarterial embolisation with two-microcatheter technique…
Figure 1
Transarterial embolisation with two-microcatheter technique of a left sigmoid sinus dural arteriovenous fistula…
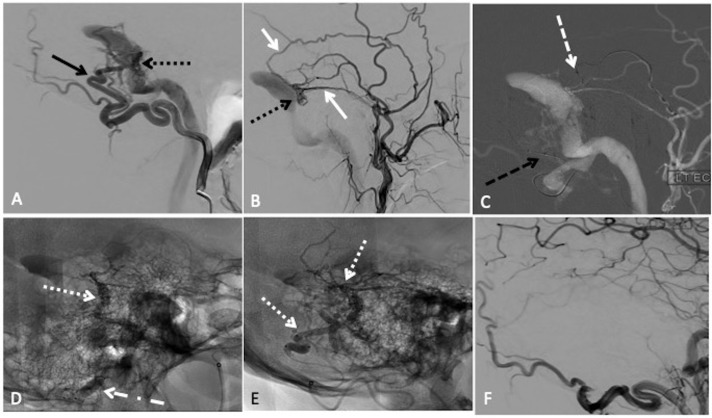
Figure 1
Transarterial embolisation with two-microcatheter technique of a left sigmoid sinus dural arteriovenous fistula (dAVF) with precipitating hydrophobic injectable liquid (PHIL). (A) Lateral projection pre-embolisation angiogram, selective left occipital artery (OA) injection and (B) left main trunk external carotid artery injection showing multiple arterial feeders arising from the OA (solid black arrow) and middle meningeal artery (MMA) (solid white arrow), draining into a common channel (dotted black arrow). (C) Lateral road map angiogram showing dual microcatheter technique with positioning of Headway Duo microcatheter within the MMA (dashed white arrow) and Scepter C 4×10 mm balloon microcatheter in the OA (dashed black arrow). (D) Unsubtracted lateral view showing PHIL cast (dotted white arrow) after single infusion through the MMA with inflation of the Scepter balloon (dotted dashed black arrow) to reduce dAVF flow. (E) Final PHIL cast (dotted white arrow) following infusion through the MMA and OA. (F) Final lateral digital subtraction angiography (DSA), left common carotid injection showing no residual dAVF.
Figure 2
Combined transarterial and transvenous embolisation…
Figure 2
Combined transarterial and transvenous embolisation of a left transverse sinus dural arteriovenous fistula…
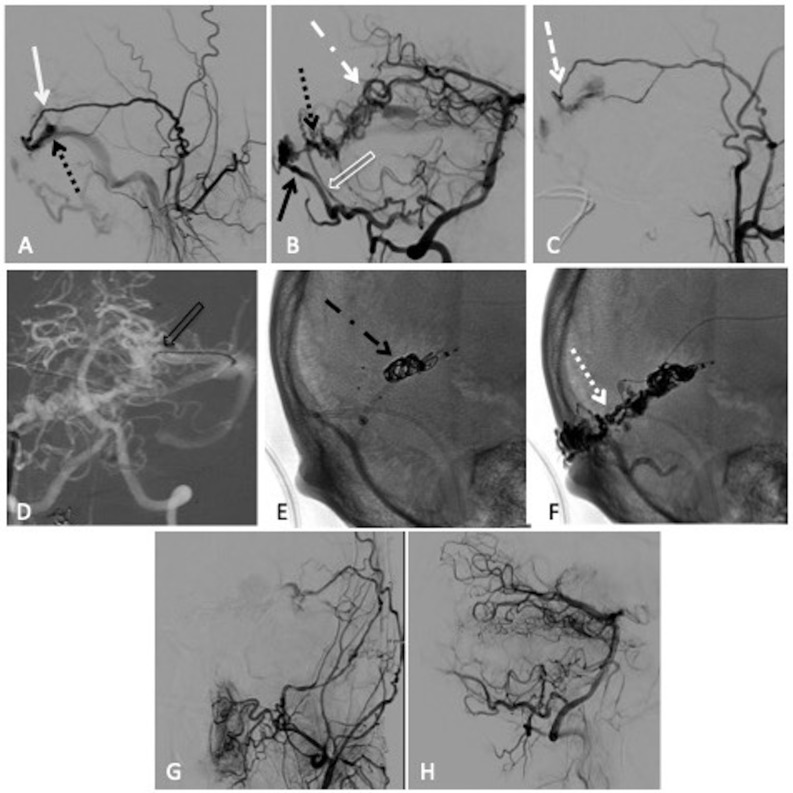
Figure 2
Combined transarterial and transvenous embolisation of a left transverse sinus dural arteriovenous fistula (dAVF) with Onyx and microcoils. (A) Lateral projection pre-embolisation angiogram, selective left external carotid artery (ECA) injection and (B) right vertebral artery (VA) injection showing multiple arterial feeders arising from the left middle meningeal artery (MMA) (solid white arrow), right occipital artery (solid black arrow), right posterior meningeal artery (clear white arrow) and left artery of Davidoff and Schechter (dotted white dashed arrow), draining into a common channel (dotted black arrow). (C) Left ECA injection showing Scepter XC 4×11 mm microcatheter positioned within the MMA (dashed white arrow). (D) Anteroposterior (AP) road map showing Echelon 14 microcatheter positioned through the left transverse sinus and within the venous pouch (clear black arrow). Unsubtracted lateral view, (E) showing successful deployment of microcoils within the venous pouch (dotted black dashed arrow), (F) showing the Onyx cast after successful infusion through the MMA (dotted white arrow). Postembolisation lateral angiogram, (G) right VA injection and (H) left common carotid artery injection showing no residual dAVF.
Sakaki T, Morimoto T, Nakase H, et al. . Dural arteriovenous fistula of the posterior fossa developing after surgical occlusion of the sigmoid sinus. Report of five cases. J Neurosurg 1996;84:113–8. 10.3171/jns.1996.84.1.0113
-
DOI
-
PubMed
McConnell KA, Tjoumakaris SI, Allen J, et al. . Neuroendovascular management of dural arteriovenous malformations. Neurosurg Clin N Am 2009;20:431–9. 10.1016/j.nec.2009.07.014
-
DOI
-
PubMed
Cognard C, Gobin YP, Pierot L, et al. . Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology 1995;194:671–80. 10.1148/radiology.194.3.7862961
-
DOI
-
PubMed
Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg 1995;82:166–79. 10.3171/jns.1995.82.2.0166
-
DOI
-
PubMed
Satomi J, van Dijk JMC, Terbrugge KG, et al. . Benign cranial dural arteriovenous fistulas: outcome of conservative management based on the natural history of the lesion. J Neurosurg 2002;97:767–70. 10.3171/jns.2002.97.4.0767
-
DOI
-
PubMed