

Pitfalls in assessing stromal tumor infiltrating lymphocytes (sTILs) in breast cancer
- PMID: 32411819
- PMCID: PMC7217863
- DOI: 10.1038/s41523-020-0156-0
Pitfalls in assessing stromal tumor infiltrating lymphocytes (sTILs) in breast cancer
Abstract
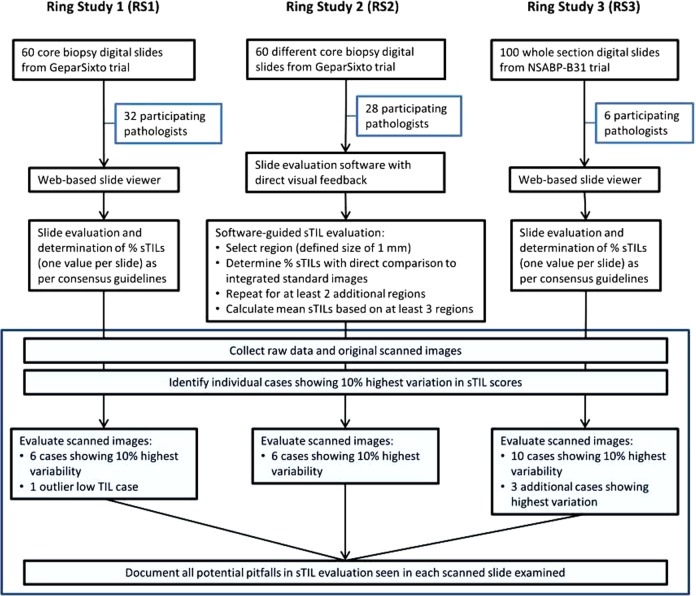
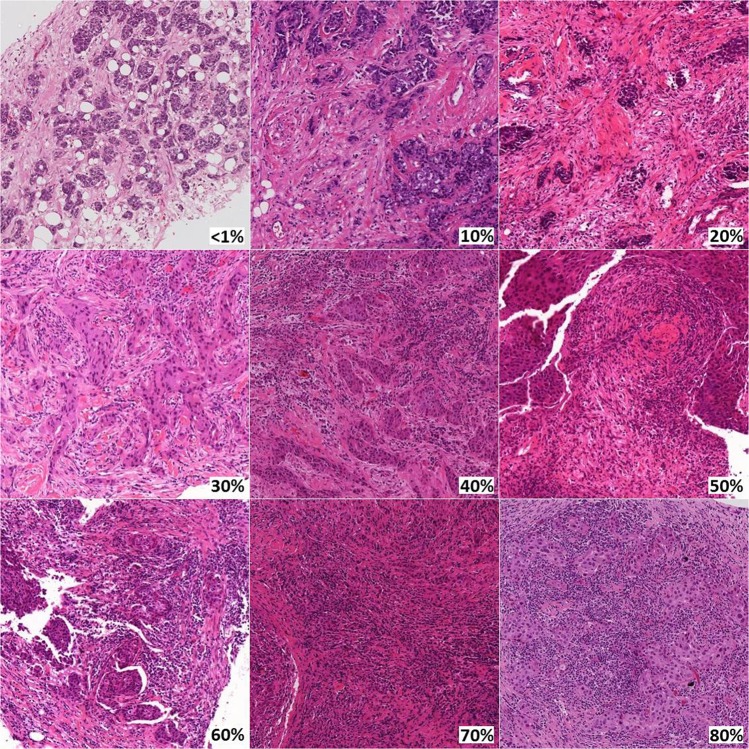
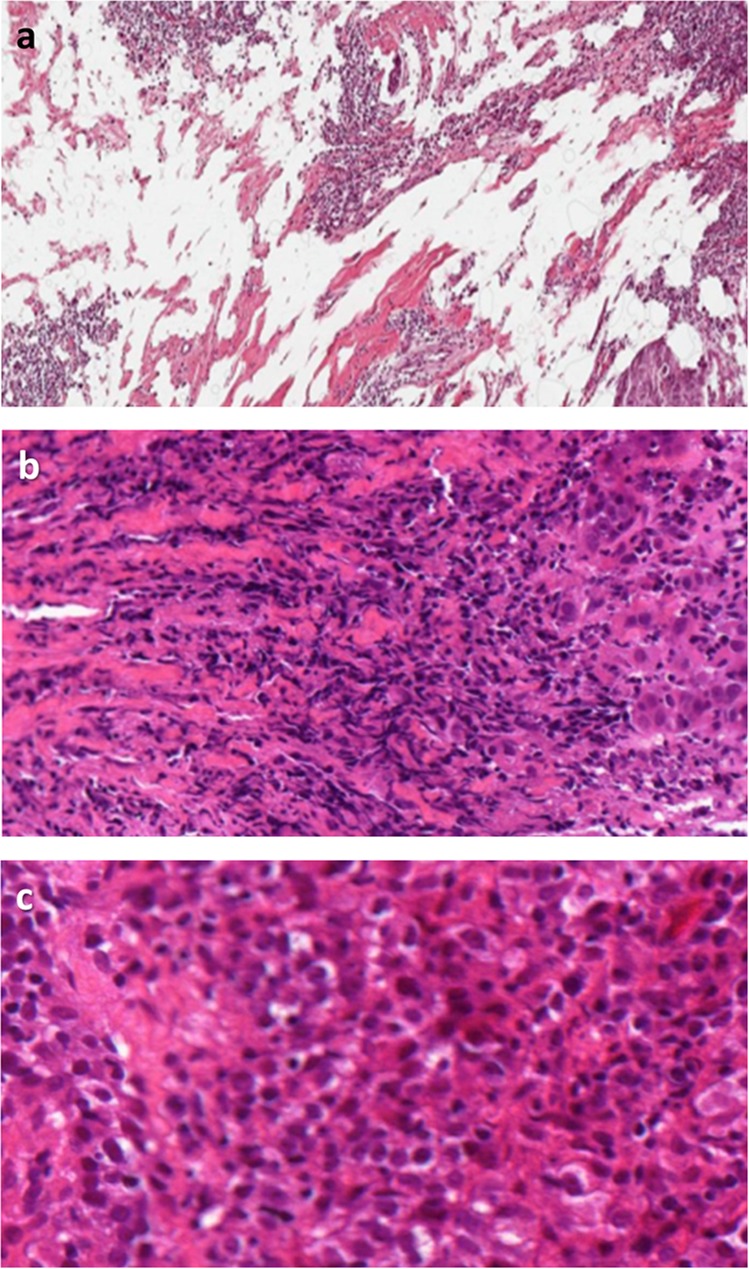
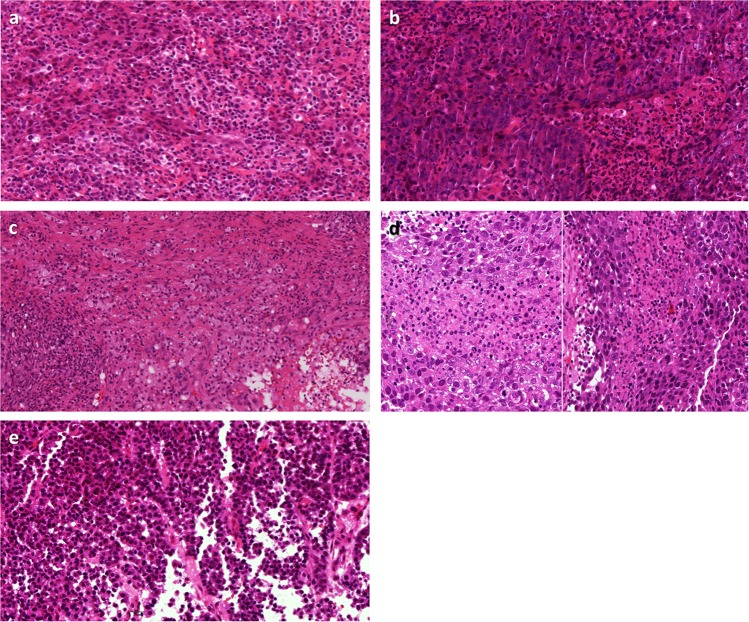
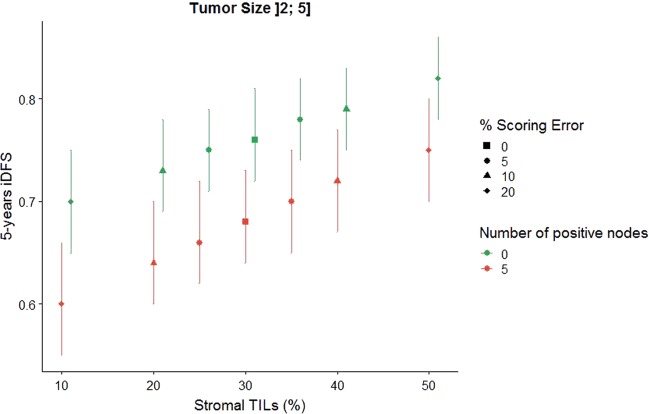
Stromal tumor-infiltrating lymphocytes (sTILs) are important prognostic and predictive biomarkers in triple-negative (TNBC) and HER2-positive breast cancer. Incorporating sTILs into clinical practice necessitates reproducible assessment. Previously developed standardized scoring guidelines have been widely embraced by the clinical and research communities. We evaluated sources of variability in sTIL assessment by pathologists in three previous sTIL ring studies. We identify common challenges and evaluate impact of discrepancies on outcome estimates in early TNBC using a newly-developed prognostic tool. Discordant sTIL assessment is driven by heterogeneity in lymphocyte distribution. Additional factors include: technical slide-related issues; scoring outside the tumor boundary; tumors with minimal assessable stroma; including lymphocytes associated with other structures; and including other inflammatory cells. Small variations in sTIL assessment modestly alter risk estimation in early TNBC but have the potential to affect treatment selection if cutpoints are employed. Scoring and averaging multiple areas, as well as use of reference images, improve consistency of sTIL evaluation. Moreover, to assist in avoiding the pitfalls identified in this analysis, we developed an educational resource available at www.tilsinbreastcancer.org/pitfalls.
Keywords: Immunosurveillance; Prognostic markers.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsA.E. is on the Roche advisory board and has reported honoraria from Amgen, Novartis and Roche. A.J.L. is a consultant for BMS, Merck, AZ/Medimmune, and Genentech. R.S. reports research funding from Roche, Puma, Merck; advisory board and consultancy for BMS; travel funding from Roche, Merck, and Astra Zeneca. S.G. reports Lab research funding from Lilly, Clinical research funding from Eli Lilly and Novartis and is a Paid advisor to Eli Lilly, Novartis, and G1 Therapeutics. J.v.d.L. is member of the scientific advisory boards of Philips, the Netherlands and ContextVision, Sweden and receives research funding from Philips, the Netherlands and Sectra, Sweden. S.A. reports Research funding to institution from Merck, Genentech, BMS, Novartis, Celgene and Amgen and is an uncompensated consultant /steering committee member for Merck, Genentech and BMS. T.O.N. has consulted for Nanostring and received compensation and has intellectual property rights/ownership interests from Bioclassifier LLC [not related to the subject material under consideration]. S.L. receives research funding to institution from Novartis, Bristol Meyers Squibb, Merck, Roche-Genentech, Puma Biotechnology, Pfizer and Eli Lilly, has acted as consultant (not compensated) to Seattle Genetics, Pfizer, Novartis, BMS, Merck, AstraZeneca and Roche-Genentech and acted as consultant (paid to her institution) to Aduro Biotech. S.R.L. has received travel and educational funding from Roche/Ventana. A.M. is an equity holder in Elucid Bioimaging and in Inspirata Inc., a scientific advisory consultant for Inspirata Inc, has served as a scientific advisory board member for Inspirata Inc, Astrazeneca, Bristol Meyers-Squibb and Merck, has sponsored research agreements with Philips and Inspirata Inc, is involved in a NIH U24 grant with PathCore Inc, and 3 different R01 grants with Inspirata Inc. and his technology has been licensed to Elucid Bioimaging and Inspirata Inc. G.C. is on the advisory boards of Roche, BMS, Pfizer, Seattle Genetics and Ellipsis, and reports personal fees from Roche, BMS, Pfizer, Seattle Genetics, and Ellipsis, outside of the submitted work. J.H. is the director and owner of Vivactiv Ltd. J.H. is the director and owner of Slide Score B.V. F.P.L. reports funding from Astrazeneca, BMS, Roche, MSD, Pfizer, Novartis, Sanofi, Eli Lilly. J.B. reports consultancies from Insight Genetics, BioNTech AG, Biotheranostics, Pfizer, RNA Diagnostics and OncoXchange, research funding from Thermo Fisher Scientific, Genoptix, Agendia, NanoString Technologies, Stratifyer GmbH and Biotheranostics, applied for patents, including Jan 2017: Methods and Devices for Predicting Anthracycline Treatment Efficacy, US utility—15/325,472; EPO—15822898.1; Canada—not yet assigned; Jan 2017: Systems, Devices and Methods for Constructing and Using a Biomarker, US utility—15/328,108; EPO—15824751.0; Canada—not yet assigned; Oct 2016: Histone gene module predicts anthracycline benefit, PCT/CA2016/000247; Dec 2016: 95‐Gene Signature of Residual Risk Following Endocrine Treatment, PCT/CA2016/000304; Dec 2016: Immune Gene Signature Predicts Anthracycline Benefit, PCT/CA2016/000305. M.A.S. reports consulting work for Achilles Therapeutics. C.S. reports receipt of grants/research support from Pfizer, AstraZeneca, BMS and Ventana; receipt of honoraria, consultancy, or SAB Member fees from Pfizer, Novartis, GlaxoSmithKline, MSD, BMS, Celgene, AstraZeneca, Illumina, Sarah Canon Research Institute, Genentech, Roche-Ventana, GRAIL, Medicxi; Advisor for Dynamo Therapeutics; Stock shareholder in Apogen Biotechnologies, Epic Bioscience, GRAIL; Co-Founder & stock options in Achilles Therapeutics. A.H.B. is the co-founder and CEO of PathAI. J.K. is an employee of PathAI. D.D. is on the advisory board for Oncology Analytics, Inc, and a consultant for Novartis. D.L.R. is on the advisory board of Amgen, Astra Zeneca, Cell Signaling Technology, Cepheid, Daiichi Sankyo, GSK, Konica/Minolta, Merck, NanoString, Perkin Elmer, Ventana, Ultivue; receives research support from Astra Zeneca, Cepheid, Navigate BioPharma, NextCure, Lilly, Ultivue; instrument support from Ventana, Akoya/Perkin Elmer, NanoString; paid consultant for Biocept; received travel honoraria from BMS, founder and equity holder for PixelGear and received royalty from Rarecyte. A.T. reports benefits from ICR’s Inventors Scheme associated with patents for one of PARP inhibitors in BRCA1/2 associated cancers, as well as honoraria from Pfizer, Vertex, Prime Oncology, Artios, honoraria and stock in InBioMotion, honoraria and financial support for research from AstraZeneca, Medivation, Myriad Genetics and Merck Serono. This work includes contributions from, and was reviewed by, individuals at the FDA. This work has been approved for publication by the agency, but it does not necessarily reflect official agency policy. Certain commercial materials and equipment are identified in order to adequately specify experimental procedures. In no case does such identification imply recommendation or endorsement by the FDA, nor does it imply that the items identified are necessarily the best available for the purpose. This work includes contributions from, and was reviewed by, individuals who received funding from the National Institutes of Health, the U.S. Department of Veterans Affairs and the Department of Defense. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the U.S. Department of Veterans Affairs, the Department of Defense, or the United States Government.
Figures




References
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- FC001202/WT_/Wellcome Trust/United Kingdom
- 28990/CRUK_/Cancer Research UK/United Kingdom
- R01 CA216579/CA/NCI NIH HHS/United States
- K12 CA090625/CA/NCI NIH HHS/United States
- MC_UP_1203/1/MRC_/Medical Research Council/United Kingdom
- C06 RR012463/RR/NCRR NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U24 CA199374/CA/NCI NIH HHS/United States
- 24869/CRUK_/Cancer Research UK/United Kingdom
- U01 CA239055/CA/NCI NIH HHS/United States
- UG3 CA225021/CA/NCI NIH HHS/United States
- FC001169/WT_/Wellcome Trust/United Kingdom
- 25351/CRUK_/Cancer Research UK/United Kingdom
- R01 CA220581/CA/NCI NIH HHS/United States
- U24 CA215109/CA/NCI NIH HHS/United States
- R01 CA208236/CA/NCI NIH HHS/United States
- R01 CA202752/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- 25223/CRUK_/Cancer Research UK/United Kingdom
- I01 BX004121/BX/BLRD VA/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
