

National and regional prevalence of posttraumatic stress disorder in sub-Saharan Africa: A systematic review and meta-analysis
- PMID: 32413027
- PMCID: PMC7228043
- DOI: 10.1371/journal.pmed.1003090
National and regional prevalence of posttraumatic stress disorder in sub-Saharan Africa: A systematic review and meta-analysis
Erratum in
-
Correction: National and regional prevalence of posttraumatic stress disorder in sub-Saharan Africa: A systematic review and meta-analysis.PLoS Med. 2020 Jul 24;17(7):e1003312. doi: 10.1371/journal.pmed.1003312. eCollection 2020 Jul. PLoS Med. 2020. PMID: 32706782 Free PMC article.
Abstract
Background: People living in sub-Saharan Africa (SSA) are disproportionately exposed to trauma and may be at increased risk for posttraumatic stress disorder (PTSD). However, a dearth of population-level representative data from SSA is a barrier to assessing PTSD. This manuscript sought to calculate pooled PTSD prevalence estimates from nationally and regionally representative surveys in SSA.
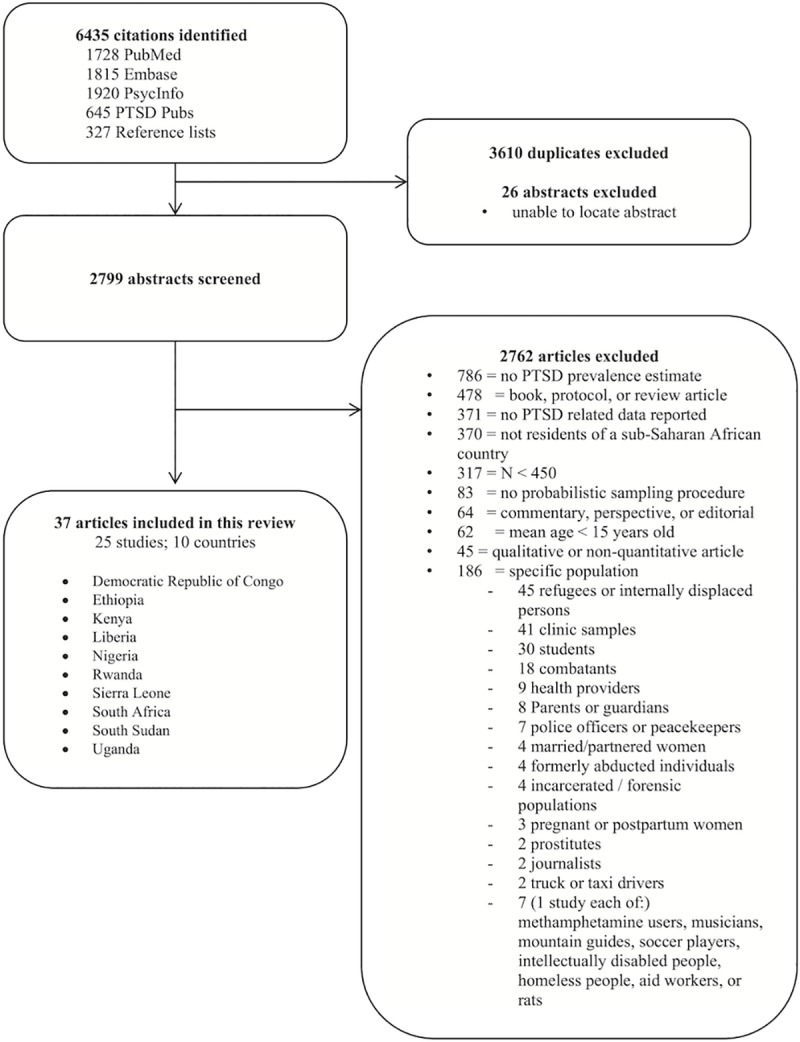
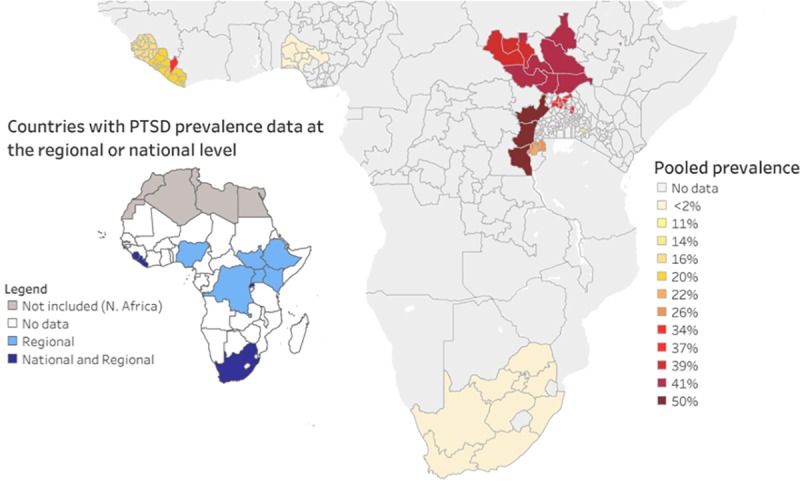
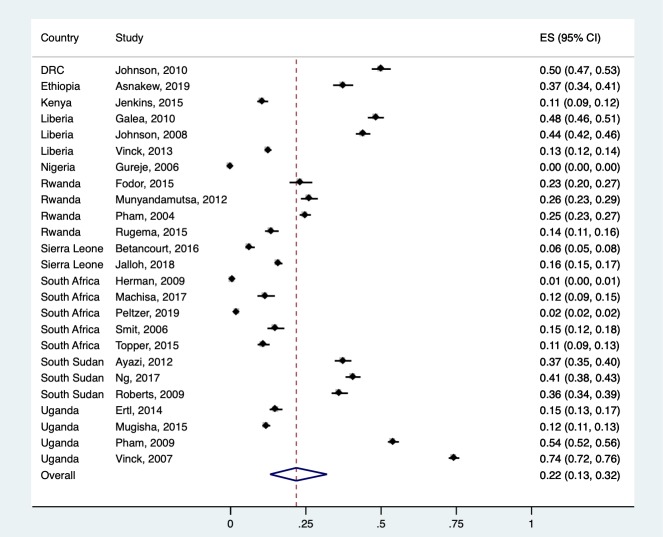
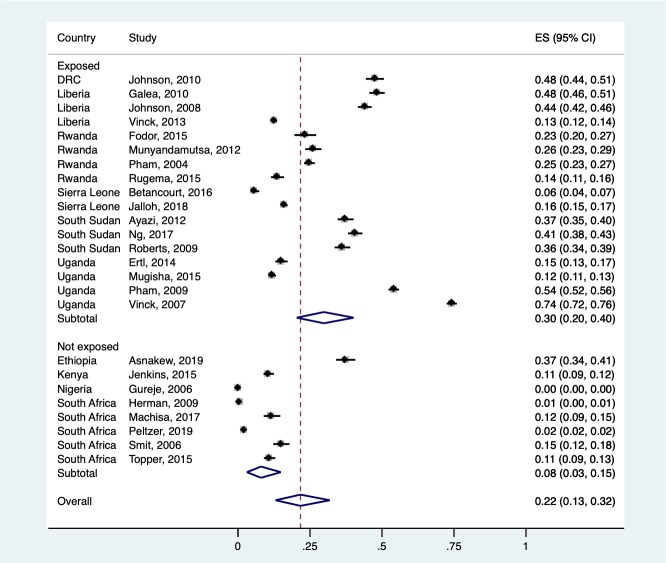
Methods and findings: The search was conducted in PubMed, Embase, PsycINFO, and PTSDpubs and was last run between October 18, 2019, and November 11, 2019. We included studies that were published in peer-reviewed journals; used probabilistic sampling methods and systematic PTSD assessments; and included ≥ 450 participants who were current residents of an SSA country, at least 50% of whom were aged between 15 and 65 years. The primary outcomes were point prevalence estimates of PTSD across all studies, and then within subgroups. The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (registration number CRD42016029441). Out of 2,825 unique articles reviewed, 25 studies including a total of 58,887 eligible participants (54% female) in 10 out of the 48 countries in SSA were identified. Most studies enrolled any adult aged 18 years or older. However, some studies only enrolled specific age brackets or persons as young as 15 years old. Six studies were national surveys, and 19 were regional. There were 4 key findings in the meta-analysis: (1) the overall pooled prevalence of probable PTSD was 22% (95% CI 13%-32%), while the current prevalence-defined as 1 week to 1 month-was 25% (95% CI 16%-36%); (2) prevalence estimates were highly variable, ranging from 0% (95% CI 0%-0%) to 74% (95% CI 72%-76%); (3) conflict-unexposed regions had a pooled prevalence of probable PTSD of 8% (95% CI 3%-15%), while conflict-exposed regions had a pooled prevalence of probable PTSD of 30% (95% CI 21%-40%; p < 0.001); and (4) there was no significant difference in the pooled prevalence of PTSD for men and women. The primary limitations of our methodology are our exclusion of the following study types: those published in languages other than English, French, and Portuguese; smaller studies; those that focused on key populations; those that reported only on continuous measures of PTSD symptoms; and unpublished or non-peer-reviewed studies.
Conclusions: In this study, PTSD symptoms consistent with a probable diagnosis were found to be common in SSA, especially in regions exposed to armed conflict. However, these studies only represent data from 10 of the 48 SSA countries, and only 6 studies provided national-level data. Given the enormous heterogeneity expected across the continent, and also within countries and regions, this review cannot speak to rates of PTSD in any regions not included in this review. Thus, substantial gaps in our knowledge of PTSD prevalence in SSA remain. More research on population-level prevalence is needed to determine the burden of trauma symptoms and PTSD in SSA and to identify acceptable and feasible approaches to address this burden given limited mental healthcare resources.
Conflict of interest statement
C.H. is a member of the Editorial Board of PLOS Medicine.
Figures
References
-
- Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–86. Epub 2013/09/03. 10.1016/S0140-6736(13)61611-6 . - DOI - PubMed
-
- Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61 Suppl 5:4–12; discussion 3–4. Epub 2000/04/13. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
