

Bridging the treatment gap in infant medulloblastoma: molecularly informed outcomes of a globally feasible regimen
- PMID: 32413139
- PMCID: PMC7746938
- DOI: 10.1093/neuonc/noaa122
Bridging the treatment gap in infant medulloblastoma: molecularly informed outcomes of a globally feasible regimen
Abstract
Background: Infant medulloblastoma represents an enormous challenge in neuro-oncology, due to their simultaneous high-risk of recurrence and high risk of severe neurodevelopmental sequelae with craniospinal irradiation. Currently infant medulloblastoma are treated with intensified protocols, either comprising intraventricular methotrexate or autologous transplant, both of which carry significant morbidity and are not feasible in the majority of the world. We sought to evaluate the molecular predictors of outcome in a cohort of infants homogeneously treated with induction chemotherapy, focal radiation and maintenance chemotherapy.
Methods: In a retrospective analysis, 29 young children treated with a craniospinal irradiation sparing strategy from Hospital Garrahan in Buenos Aires were profiled using Illumina HumanMethylationEPIC arrays, and correlated with survival.
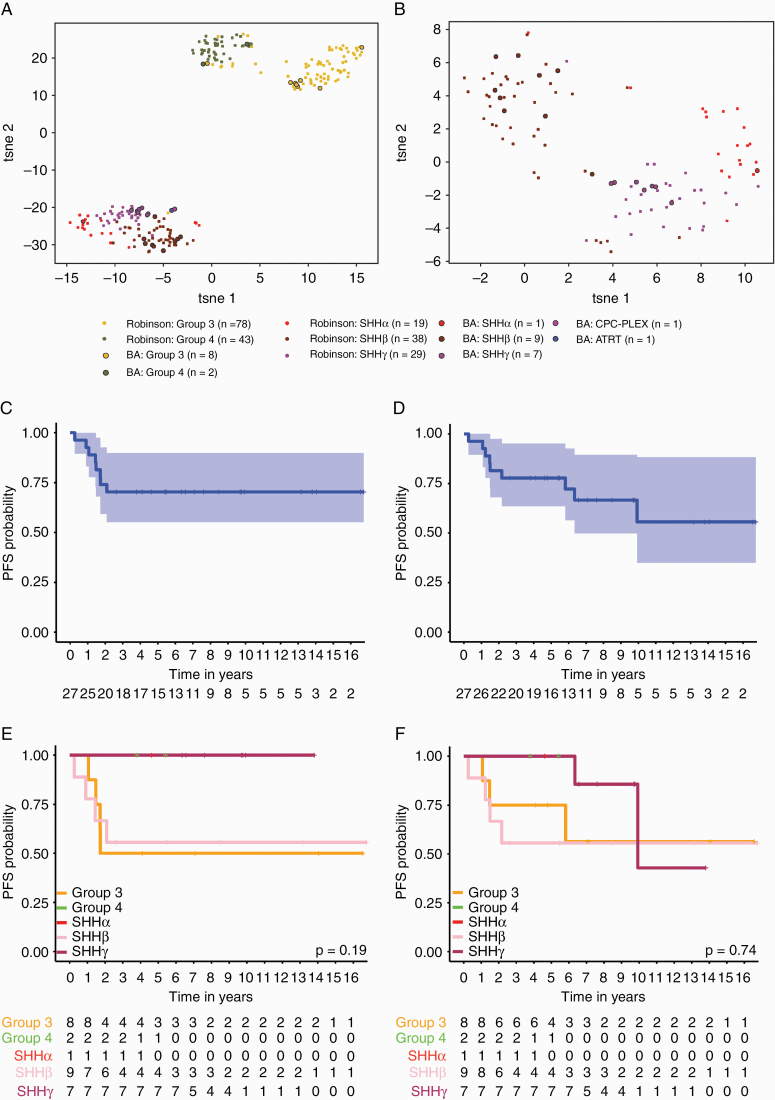
Results: Twenty-nine children (range, 0.3-4.6 y) were identified, comprising 17 sonic hedgehog (SHH), 10 Group 3/4, and 2 non-medulloblastomas. Progression-free survival (PFS) across the entire cohort was 0.704 (95% CI: 0.551-0.899). Analysis by t-distributed stochastic neighbor embedding revealed 3 predominant groups, SHHβ, SHHγ, and Group 3. Survival by subtype was highly prognostic with SHHγ having an excellent 5-year PFS of 100% (95% CI: 0.633-1) and SHHβ having a PFS of 0.56 (95% CI: 0.42-1). Group 3 had a PFS of 0.50 (95% CI: 0.25-1). Assessment of neurocognitive outcome was performed in 11 patients; the majority of survivors fell within the low average to mild intellectual disability, with a median IQ of 73.5.
Conclusions: We report a globally feasible and effective strategy avoiding craniospinal radiation in the treatment of infant medulloblastoma, including a robust molecular correlation along with neurocognitive outcomes.
Keywords: SHH; brain tumor; infant; medulloblastoma; radiation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Rutkowski S, Cohen B, Finlay J, et al. . Medulloblastoma in young children. Pediatr Blood Cancer. 2010;54(4):635–637. - PubMed
-
- Duffner PK, Horowitz ME, Krischer JP, et al. . Postoperative chemotherapy and delayed radiation in children less than three years of age with malignant brain tumors. N Engl J Med. 1993;328(24):1725–1731. - PubMed
-
- Kiltie AE, Lashford LS, Gattamaneni HR. Survival and late effects in medulloblastoma patients treated with craniospinal irradiation under three years old. Med Pediatr Oncol. 1997;28(5):348–354. - PubMed
-
- Duffner PK. Long-term effects of radiation therapy on cognitive and endocrine function in children with leukemia and brain tumors. Neurologist. 2004;10(6):293–310. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
