

The impact of the Tracey judgment on the rates and outcomes of in-hospital cardiac arrests in UK hospitals participating in the National Cardiac Arrest Audit
- PMID: 32414723
- PMCID: PMC7354039
- DOI: 10.7861/clinmed.2019-0454
The impact of the Tracey judgment on the rates and outcomes of in-hospital cardiac arrests in UK hospitals participating in the National Cardiac Arrest Audit
Abstract
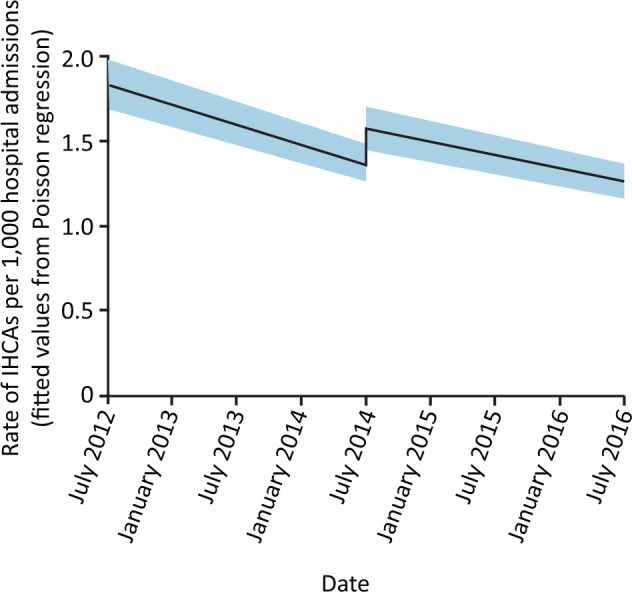
Aims: The aim was to determine if the 17 June 2014 Tracey judgment regarding 'do not attempt cardiopulmonary resuscitation' decisions led to increases in the rate of in-hospital cardiac arrests resulting in a resuscitation attempt (IHCA) and/or proportion of resuscitation attempts deemed futile.
Method: Using UK National Cardiac Arrest Audit data, the IHCA rate and proportion of resuscitation attempts deemed futile were compared for two periods (pre-judgment (01 July 2012 - 16 June 2014, inclusive) and post-judgment (01 July 2014 - 30 June 2016, inclusive)) using interrupted time series analyses.
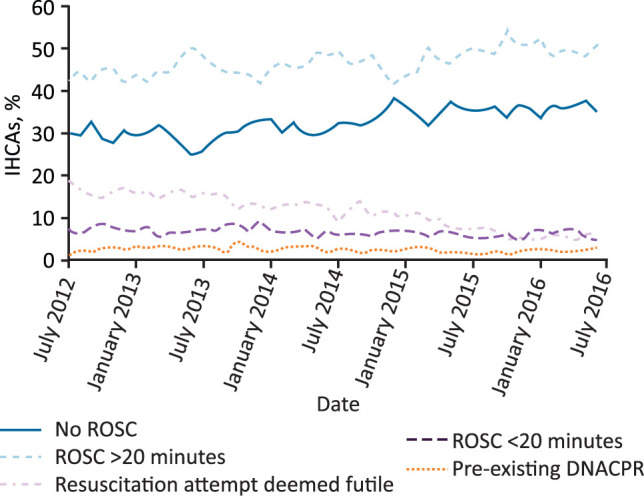
Results: A total of 43,109 IHCAs (115 hospitals) were analysed. There were fewer IHCAs post- than pre-judgment (21,324 vs 21,785, respectively). The IHCA rate was declining over time before the judgment but there was an abrupt and statistically significant increase in the period immediately following the judgment (p<0.001). This was not sustained post-judgment. The proportion of resuscitation attempts deemed futile was smaller post-judgment than pre-judgment (8.2% vs 14.9%, respectively). The rate of attempts deemed futile decreased post-judgment (p<0.001).
Conclusion: The IHCA rate increased immediately after the Tracey judgment while the proportion of resuscitation attempts deemed futile decreased. The precise mechanisms for these changes are unclear.
Keywords: DNACPR; Resuscitation; Tracey judgment; cardiac arrest; do not attempt cardiopulmonary resuscitation.
© Royal College of Physicians 2020. All rights reserved.
Figures

Similar articles
-
Peri-operative decisions about cardiopulmonary resuscitation among adults as reported to the 7th National Audit Project of the Royal College of Anaesthetists.Anaesthesia. 2024 Feb;79(2):186-192. doi: 10.1111/anae.16179. Epub 2023 Nov 22. Anaesthesia. 2024. PMID: 37991058
-
Impact of the COVID-19 pandemic on in-hospital cardiac arrests in the UK.Resuscitation. 2022 Apr;173:4-11. doi: 10.1016/j.resuscitation.2022.02.007. Epub 2022 Feb 10. Resuscitation. 2022. PMID: 35151777 Free PMC article.
-
In-hospital cardiac arrest survival before and after the COVID-19 pandemic: Have higher performing hospitals stayed high-performing?Resuscitation. 2024 Oct;203:110374. doi: 10.1016/j.resuscitation.2024.110374. Epub 2024 Aug 20. Resuscitation. 2024. PMID: 39174001
-
In-hospital cardiac arrest: the state of the art.Crit Care. 2022 Dec 6;26(1):376. doi: 10.1186/s13054-022-04247-y. Crit Care. 2022. PMID: 36474215 Free PMC article. Review.
-
Trends in In-Hospital Cardiac Arrest and Mortality Among Children With Cardiac Disease in the Intensive Care Unit: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 Feb 1;6(2):e2256178. doi: 10.1001/jamanetworkopen.2022.56178. JAMA Netw Open. 2023. PMID: 36763356 Free PMC article.
Cited by
-
COVID-19: the physician's response in the first phase.Clin Med (Lond). 2020 May;20(3):237. doi: 10.7861/clinmed.ed.20.3.1. Clin Med (Lond). 2020. PMID: 32414714 Free PMC article. No abstract available.
References
-
- R (Tracey) v Cambridge University Hospitals NHS Foundation Trust & Others: [2014] EWCA Civ 822. Royal Courts of Justice, 2014. www.judiciary.uk/wp-content/uploads/2014/06/tracey-approved.pdf [Accessed 11 March 2019].
-
- Mockford C, Fritz Z, George R, et al. Do not attempt cardiopulmonary resuscitation (DNACPR) orders: A systematic review of the barriers and facilitators of decision-making and implementation. Resuscitation 2015;88:99–113. - PubMed
-
- Nicolasora N, Pannala R, Mountantonakis S, et al. If asked, hospitalized patients will choose whether to receive life-sustaining therapies. J Hosp Med 2006;1:161–7. - PubMed
-
- Gorton AJ, Jayanthi NVG, Lepping P, Scriven MW. Patients’ attitudes towards ‘do not attempt resuscitation’ status. J Med Ethics 2008;34:624–6. - PubMed
-
- Giles H, Moule P. Do not attempt resuscitation’ decision-making: a study exploring the attitudes and experiences of nurses. Nurs Crit Care 2004;9:115–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
