

Rate and Determinants of Excessive Fat-Free Mass Loss After Bariatric Surgery
- PMID: 32415634
- PMCID: PMC7305251
- DOI: 10.1007/s11695-020-04654-6
Rate and Determinants of Excessive Fat-Free Mass Loss After Bariatric Surgery
Abstract
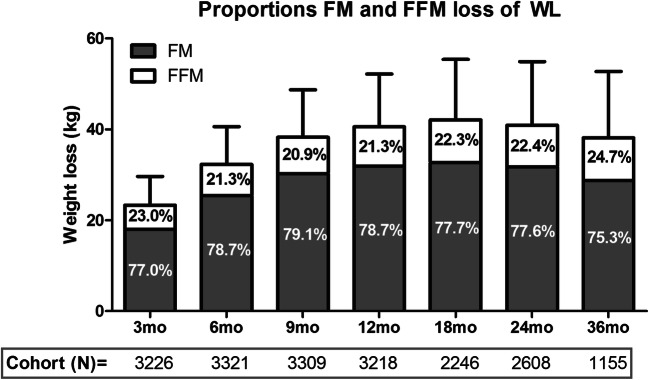
Purpose: Fat-free mass (FFM) loss is a concerning aspect of bariatric surgery, but little is known about its time-course and factors related with excessive FFM loss. This study examined (i) the progress of FFM loss up to 3 years post-bariatric surgery and (ii) the prevalence and determinants of excessive FFM loss.
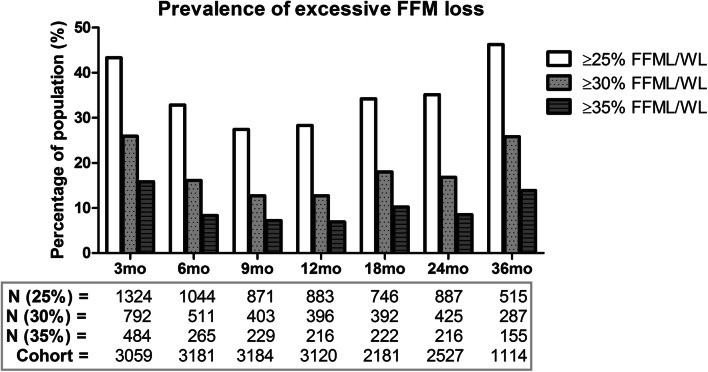
Materials and methods: A total of 3596 patients (20% males, 43.5 ± 11.1 years old, BMI = 44.2 ± 5.5 kg/m2) underwent sleeve gastrectomy (SG) or Roux-en-Y gastric bypass (RYGB) surgery. Bioelectrical impedance analysis was performed preoperatively and 3, 6, 9, 12, 18, 24 and 36 months post-surgery. Changes in body composition were assessed by mixed model analysis. Prevalence of excessive FFM loss (based on three different cutoff values: ≥ 25%, ≥ 30% and ≥ 35% FFM loss/weight loss (= %FFML/WL)) was estimated and its determinants were assessed by linear regression analysis.
Results: Highest rates of FFM loss were found at 3 and 6 months post-surgery, reflecting 57% and 73% of peak FFM loss, respectively. Prevalence of excessive FFM loss ranged from 14 to 46% at 36 months post-surgery, with an older age (β = 0.14, 95%CI = 0.10-0.18, P < .001), being male (β = 3.99, 95%CI = 2.86-5.12, P < .001), higher BMI (β = 0.13, 95%CI = 0.05-0.20, P = .002) and SG (β = 2.56, 95%CI = 1.36-3.76, P < .001) as determinants for a greater %FFML/WL.
Conclusion: Patients lost most FFM within 3 to 6 months post-surgery. Prevalence of excessive FFM loss was high, emphasizing the need for more vigorous approaches to counteract FFM loss. Furthermore, future studies should assess habitual physical activity and dietary intake shortly after surgery in relation to FFM loss.
Keywords: Bariatric surgery; Body composition; Fat-free mass.
Conflict of interest statement
MAH Nuijten declares that she has no conflict of interest. VM Monpellier works as research coordinator at the Nederlandse Obesitas Kliniek. TMH Eijsvogels declares that he has no conflict of interest. IMC Janssen is medical director of the Nederlandse Obesitas Kliniek. EJ Hazebroek declares that he has no conflict of interest. MTE Hopman declares that she has no conflict of interest.
Figures

References
-
- de Freitas Junior WR, Ilias EJ, Kassab P, Cordts R, Porto PG, Martins Rodrigues FC, et al. Assessment of the body composition and the loss of fat-free mass through bioelectric impedance analysis in patients who underwent open gastric bypass. ScientificWorldJournal. 2014;2014:843253. doi: 10.1155/2014/843253. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
