

Salt wasting syndrome in brain trauma patients: a pathophysiologic approach using sodium balance and urinary biochemical analysis
- PMID: 32416729
- PMCID: PMC7229604
- DOI: 10.1186/s12883-020-01771-8
Salt wasting syndrome in brain trauma patients: a pathophysiologic approach using sodium balance and urinary biochemical analysis
Abstract
Background: To explore the underlying mechanisms leading to the occurrence of hyponatremia and enhanced urinary sodium excretion in brain trauma patients using sodium balance and urinary biochemical analysis.
Methods: We conducted a retrospective analysis of a local database prospectively collected in 60 brain trauma patients without chronic renal dysfunction. Metabolic and hemodynamic parameters were averaged over three consecutive periods over the first seven days after admission. The main outcome investigated in this study was the occurrence of at least one episode of hyponatremia.
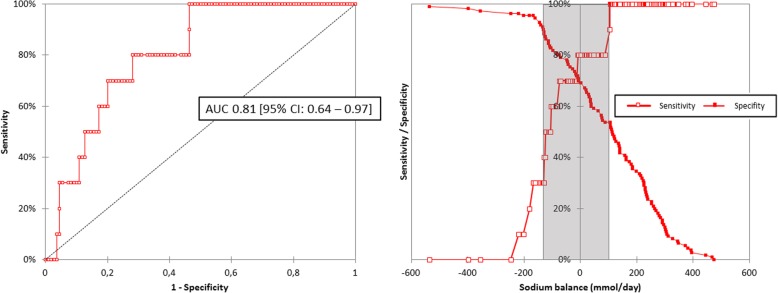
Results: Over the study period, there was a prompt decrease in sodium balance (163 ± 193 vs. -12 ± 154 mmol/day, p < 0.0001) and free water clearance (- 0.7 ± 0.7 vs. -1.8 ± 2.3 ml/min, p < 0.0001). The area under the ROC curves for sodium balance in predicting the occurrence of hyponatremia during the next period was 0.81 [95% CI: 0.64-0.97]. Variables associated with averaged urinary sodium excretion were sodium intake (R2 = 0.26, p < 0.0001) and fractional excretion of urate (R2 = 0.15, p = 0.009). Urinary sodium excretion was also higher in patients with sustained augmented renal clearance over the study period (318 ± 106 vs. 255 ± 135 mmol/day, p = 0.034).
Conclusion: The decreased vascular volume resulting from a negative sodium balance is a major precipitating factor of hyponatremia in brain trauma patients. Predisposing factors for enhanced urinary sodium excretion were high sodium intake, high fractional excretion of urate and augmented renal clearance over the first seven days after ICU admission.
Keywords: Augmented renal clearance; Brain trauma; Hyponatremia; Intensive care; Salt wasting syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Augmented Renal Clearance, Muscle Catabolism and Urinary Nitrogen Loss: Implications for Nutritional Support in Critically Ill Trauma Patients.Nutrients. 2021 Oct 11;13(10):3554. doi: 10.3390/nu13103554. Nutrients. 2021. PMID: 34684555 Free PMC article.
-
Early inhibition of natriuresis suppresses symptomatic cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage.Cerebrovasc Dis. 2013;35(2):131-7. doi: 10.1159/000346586. Epub 2013 Feb 7. Cerebrovasc Dis. 2013. PMID: 23406891
-
Body salt and water balances in cardiothoracic surgery patients with intensive care unit-acquired hyponatremia.J Crit Care. 2013 Dec;28(6):1114.e1-5. doi: 10.1016/j.jcrc.2013.05.017. Epub 2013 Jul 24. J Crit Care. 2013. PMID: 23890940
-
Is it cerebral or renal salt wasting?Kidney Int. 2009 Nov;76(9):934-8. doi: 10.1038/ki.2009.263. Epub 2009 Jul 29. Kidney Int. 2009. PMID: 19641485 Review.
-
Acute hyponatremia in the perioperative period: insights into its pathophysiology and recommendations for management.Clin Nephrol. 1998 Dec;50(6):352-60. Clin Nephrol. 1998. PMID: 9877108 Review.
Cited by
-
Augmented Renal Clearance: Prevalence, Risk Factors and Underlying Mechanism in Critically Ill Patients with Subarachnoid Hemorrhage.Neurocrit Care. 2025 Jun;42(3):878-884. doi: 10.1007/s12028-024-02144-6. Epub 2024 Nov 7. Neurocrit Care. 2025. PMID: 39511114
-
Augmented Renal Clearance, Muscle Catabolism and Urinary Nitrogen Loss: Implications for Nutritional Support in Critically Ill Trauma Patients.Nutrients. 2021 Oct 11;13(10):3554. doi: 10.3390/nu13103554. Nutrients. 2021. PMID: 34684555 Free PMC article.
-
LC-MS/MS-Based Serum Metabolomics and Transcriptome Analyses for the Mechanism of Augmented Renal Clearance.Int J Mol Sci. 2023 Jun 21;24(13):10459. doi: 10.3390/ijms241310459. Int J Mol Sci. 2023. PMID: 37445637 Free PMC article.
-
Augmented Renal Clearance: What Have We Known and What Will We Do?Front Pharmacol. 2021 Nov 2;12:723731. doi: 10.3389/fphar.2021.723731. eCollection 2021. Front Pharmacol. 2021. PMID: 34795579 Free PMC article. Review.
-
Pharmacokinetic variability and significance of therapeutic drug monitoring for broad-spectrum antimicrobials in critically ill patients.J Pharm Health Care Sci. 2025 Mar 17;11(1):21. doi: 10.1186/s40780-025-00425-6. J Pharm Health Care Sci. 2025. PMID: 40098009 Free PMC article. Review.
References
-
- Legrand M, Sonneville R. Understanding the renal response to brain injury. Intensive Care Med. 2019;45(8):1112–1115. - PubMed
-
- Audibert G, Steinmann G, de Talancé N, et al. Endocrine response after severe subarachnoid hemorrhage related to sodium and blood volume regulation. Anesth Analg. 2009;108(6):1922–1928. - PubMed
-
- Geeraerts T, Velly L, Abdennour L, et al. Management of severe traumatic brain injury (first 24hours) Anaesth Crit Care Pain Med. 2018;37(2):171–186. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
