

Management of acute kidney injury in patients with COVID-19
- PMID: 32416769
- PMCID: PMC7255232
- DOI: 10.1016/S2213-2600(20)30229-0
Management of acute kidney injury in patients with COVID-19
Abstract
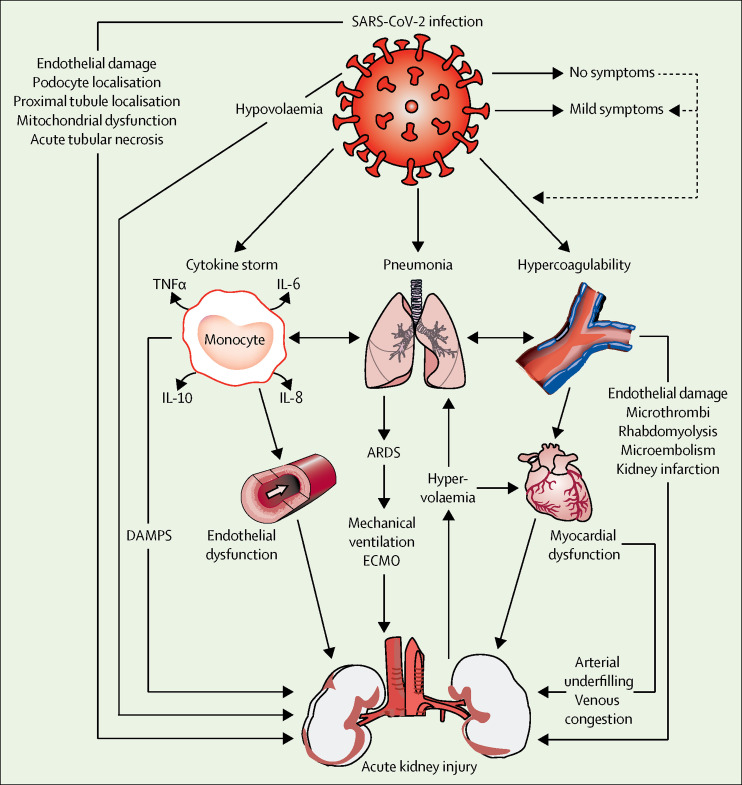
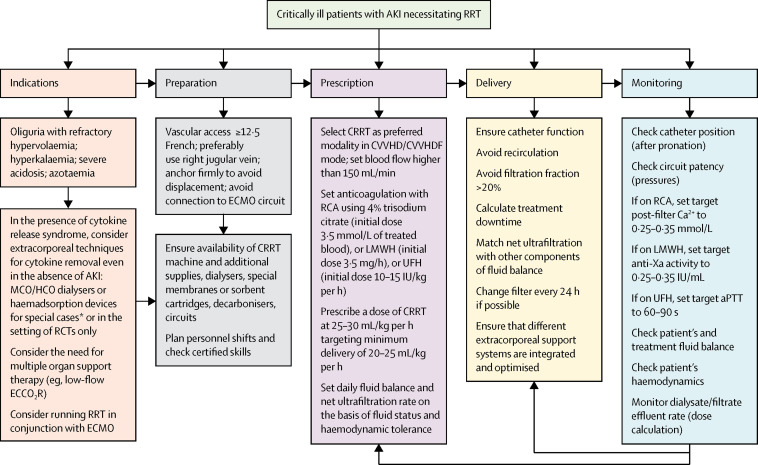
The outbreak of coronavirus disease 2019 (COVID-19) has rapidly evolved into a global pandemic. Most patients with COVID-19 have mild symptoms, but about 5% develop severe symptoms, which can include acute respiratory distress syndrome, septic shock, and multiple organ failure. Kidney involvement is frequent, with clinical presentation ranging from mild proteinuria to progressive acute kidney injury (AKI) necessitating renal replacement therapy (RRT). An understanding of the pathophysiology and mechanisms of kidney damage and AKI in the setting of critical illness and COVID-19 is emerging, although further research is needed to identify patients at risk of AKI and to guide management strategies. As no specific treatment options exist for AKI secondary to COVID-19, intensive care is largely supportive. Current approaches to prevention and management of AKI, and identification of potential indications for use of RRT and sequential extracorporeal therapies, are based mainly on clinical experience, and AKI strategies are adapted empirically to patients with COVID-19. International collaborative and cross-disciplinary research is needed to obtain adequate evidence to support current clinical approaches and to develop new approaches to management.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
References
-
- Acute kidney injury in COVID-19 patients. ESICMtv Webinar. Posted April 17, 2020. https://www.esicm.org/blog/?p=2789
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
