

Chronic Immune Activation in TB/HIV Co-infection
- PMID: 32417227
- PMCID: PMC7390597
- DOI: 10.1016/j.tim.2020.03.015
Chronic Immune Activation in TB/HIV Co-infection
Erratum in
-
Chronic Immune Activation in TB/HIV Co-infection: (Trends in Microbiology 28, 619-632; 2020).Trends Microbiol. 2020 Aug;28(8):699. doi: 10.1016/j.tim.2020.05.006. Epub 2020 May 29. Trends Microbiol. 2020. PMID: 32482557 No abstract available.
Abstract
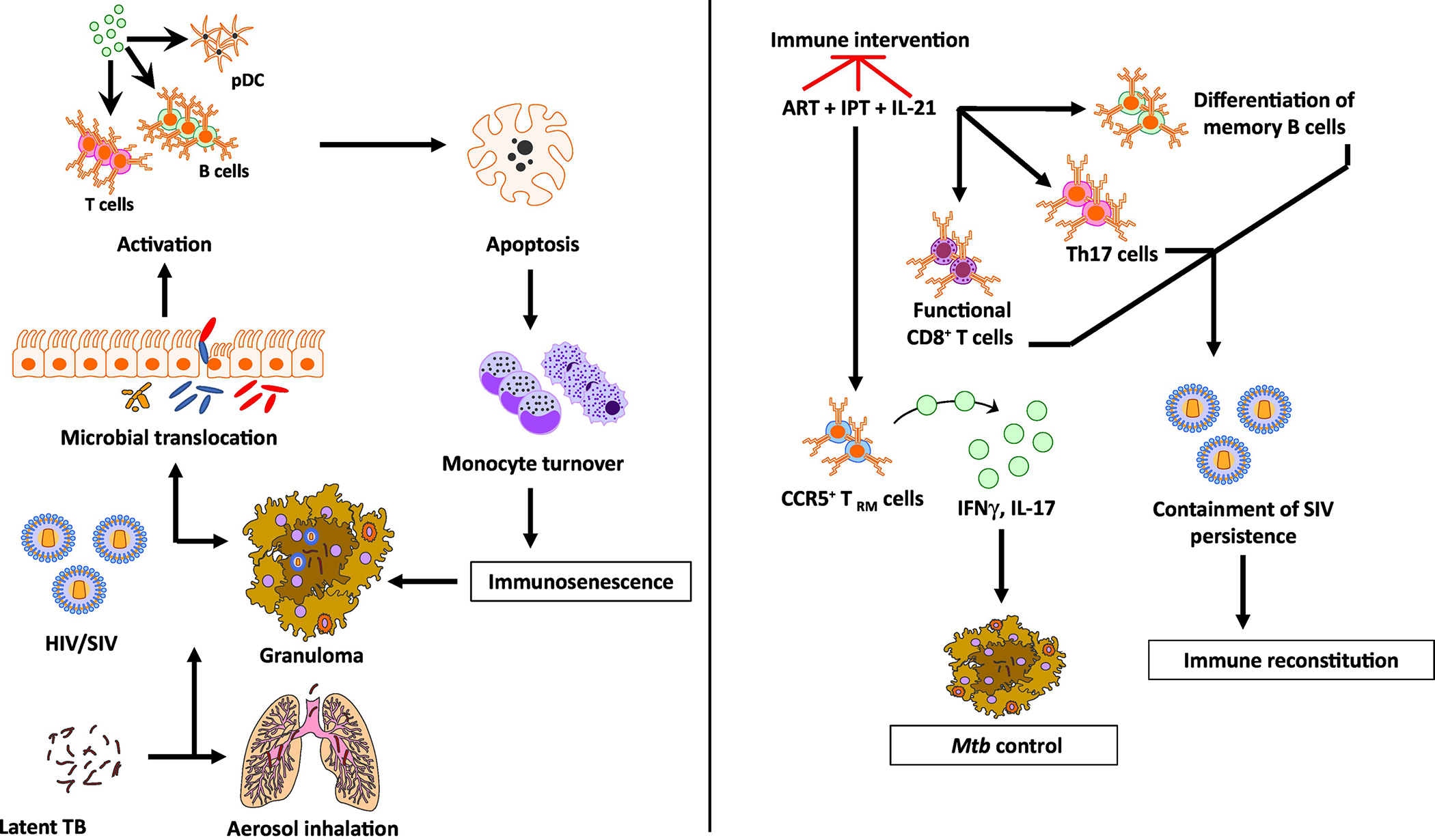
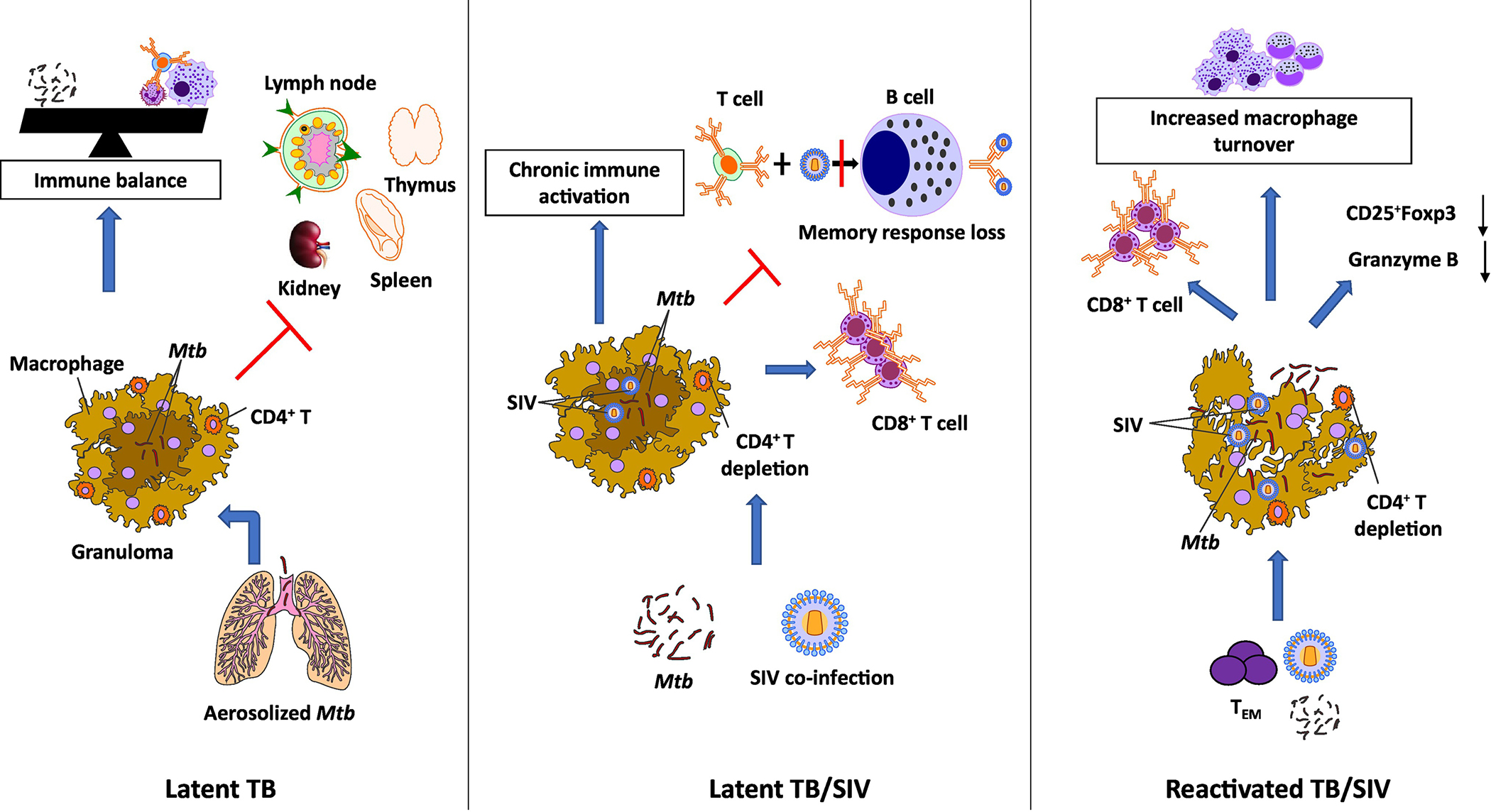
HIV co-infection is the most critical risk factor for the reactivation of latent tuberculosis (TB) infection (LTBI). While CD4+ T cell depletion has been considered the major cause of HIV-induced reactivation of LTBI, recent work in macaques co-infected with Mycobacterium tuberculosis (Mtb)/simian immunodeficiency virus (SIV) suggests that cytopathic effects of SIV resulting in chronic immune activation and dysregulation of T cell homeostasis correlate with reactivation of LTBI. This review builds on compelling data that the reactivation of LTBI during HIV co-infection is likely to be driven by the events of HIV replication and therefore highlights the need to have optimum translational interventions directed at reactivation due to co-infection.
Keywords: Mtb; SIV; chronic immune activation; co-infection; nonhuman primates.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
