

Immune checkpoint inhibitor-related colitis assessment and prognosis: can IBD scoring point the way?
- PMID: 32418993
- PMCID: PMC7374736
- DOI: 10.1038/s41416-020-0882-y
Immune checkpoint inhibitor-related colitis assessment and prognosis: can IBD scoring point the way?
Abstract
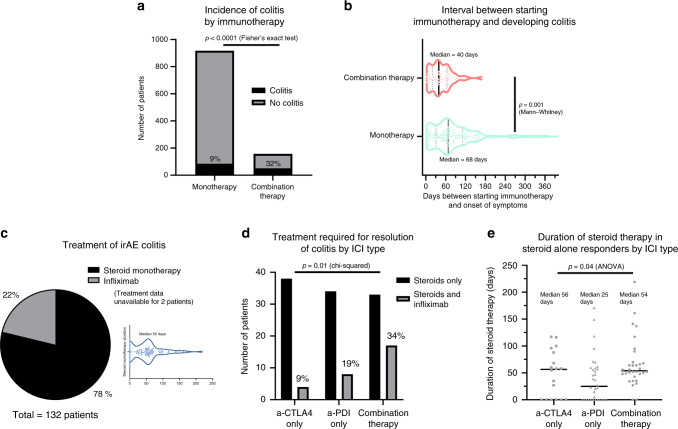
Background: Immune checkpoint inhibitors (ICI) improve survival but cause immune-related adverse events (irAE). We sought to determine if CTCAE classification, IBD biomarkers/endoscopic/histological scores correlate with irAE colitis outcomes.
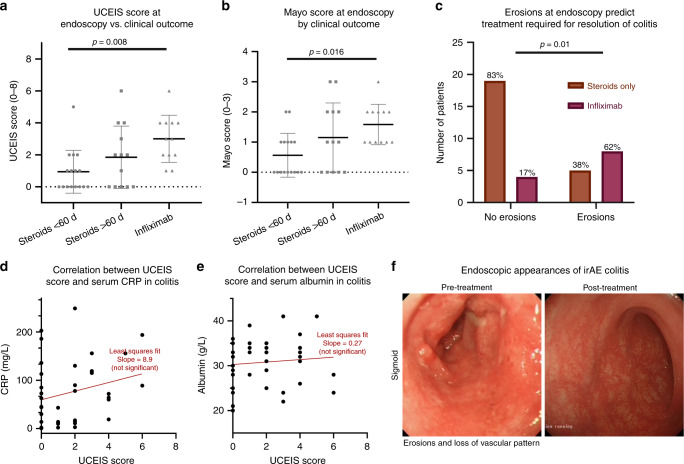
Methods: A dual-centre retrospective study was performed on patients receiving ICI for melanoma, NSCLC or urothelial cancer from 2012 to 2018. Demographics, clinical data, endoscopies (reanalysed using Mayo/Ulcerative Colitis Endoscopic Index of Severity (UCEIS) scores), histology (scored with Nancy Index) and treatment outcomes were analysed.
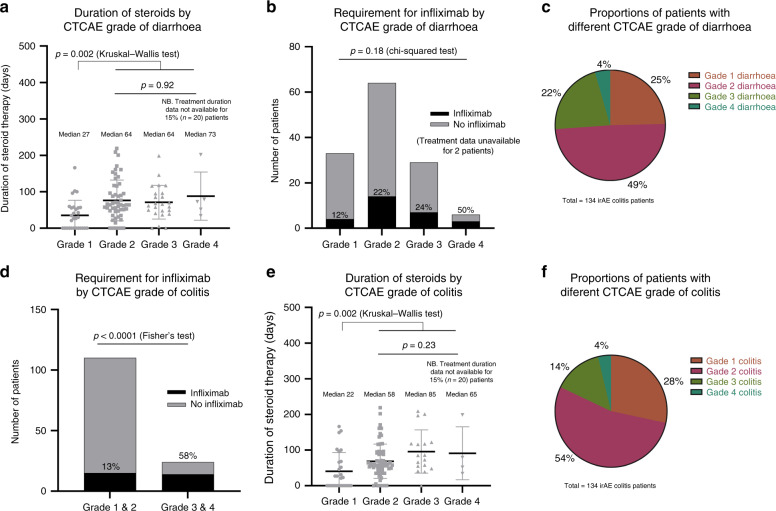
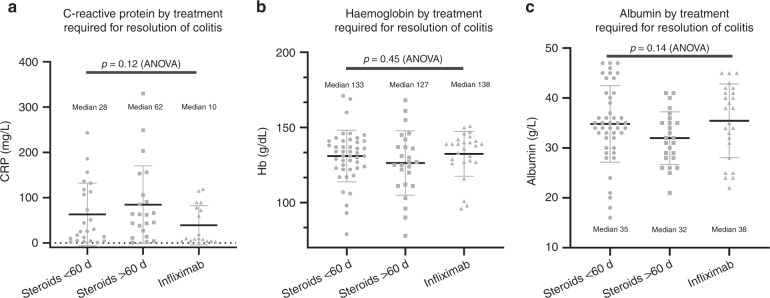
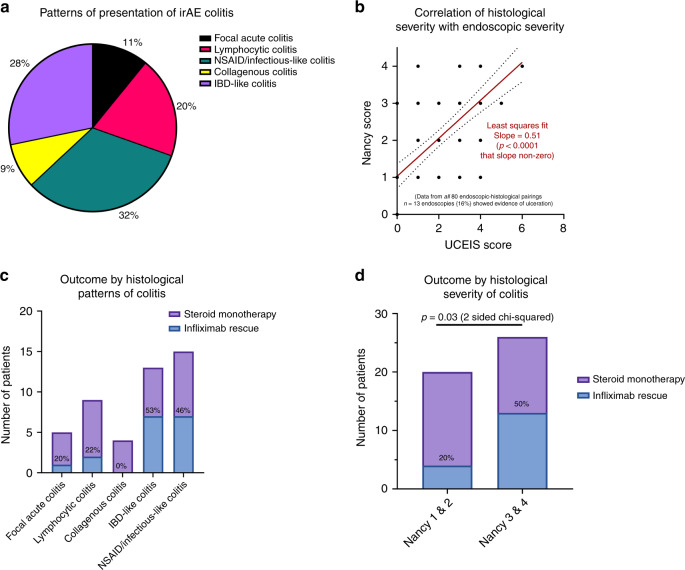
Results: In all, 1074 patients were analysed. Twelve percent (134) developed irAE colitis. Median patient age was 66, 59% were male. CTCAE diarrhoea grade does not correlate with steroid/ infliximab use. G3/4 colitis patients are more likely to need infliximab (p < 0.0001) but colitis grade does not correlate with steroid duration. CRP, albumin and haemoglobin do not correlate with severity. The UCEIS (p = 0.008) and Mayo (p = 0.016) scores correlate with severity/infliximab requirement. Patients with higher Nancy indices (3/4) are more likely to require infliximab (p = 0.03).
Conclusions: CTCAE assessment does not accurately reflect colitis severity and our data do not support its use in isolation, as this may negatively impact timely management. Our data support utilising endoscopic scoring for patients with >grade 1 CTCAE disease, and demonstrate the potential prognostic utility of objective histologic scoring.
Conflict of interest statement
V.T.F.C. has received speaker fees from Janssen. A.O.-B. is an MRC Clinical Training Fellow based at the University of Liverpool supported by the North West England Medical Research Council Fellowship Scheme in Clinical Pharmacology and Therapeutics, which is funded by the Medical Research Council, Roche Pharma, Eli Lilly and Company Limited, UCB Pharma, Novartis, the University of Liverpool and the University of Manchester. She has received honoraria for speaking at educational events from Roche Pharma, Bristol-Myers-Squibb (BMS) and MSD. She has received honoraria for attending BMS advisory boards. J.J.S. has received speaker fees from BMS and Pierre Fabre; acted as a consultant for BMS, MSD, Amgen, Delcath and Immunocore; and his institution has received research grants from BMS and AZ. M.P. is the director of the North West England Medical Research Council Fellowship Scheme in Clinical Pharmacology and Therapeutics. M.R.M. has acted as a consultant for Amgen, AstraZeneca, Bristol-Myers Squibb, Eisai, GlaxoSmithKline, Immunocore, Lilly, Merck, Millennium, Novartis, Physiomics, Rigontec, and Roche; his institution has received research grants from Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Clovis, Eisai, GlaxoSmithKline, Immunocore, Merck, Millennium, Novartis, Pfizer, Rigontec, Roche, and Vertex. O.B. has received speaker fees from BMS and has received a research grant from Celgene. M.T. has performed Advisory/Consultancy work for Pfizer, Novartis, Lilly, Janssen, Roche, Vaccitech, BMS, and has been a paid speaker for and received paid speaking engagements and education support from Novartis, Pfizer, Roche, Janssen, BMS, Genomic Health, Astellas, Esai, Everything Genetics. A.P. has received honoraria from Ipsen, Roche Bayer, Merck and BMC; and has received non-financial support from Ipsen and grants from Merck. The other authors have no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
