

Resuscitation of the patient with suspected/confirmed COVID-19 when wearing personal protective equipment: A randomized multicenter crossover simulation trial
- PMID: 32419128
- PMCID: PMC8078983
- DOI: 10.5603/CJ.a2020.0068
Resuscitation of the patient with suspected/confirmed COVID-19 when wearing personal protective equipment: A randomized multicenter crossover simulation trial
Abstract
Background: The aim of the study was to evaluate various methods of chest compressions in patients with suspected/confirmed SARS-CoV-2 infection conducted by medical students wearing full personal protective equipment (PPE) for aerosol generating procedures (AGP).
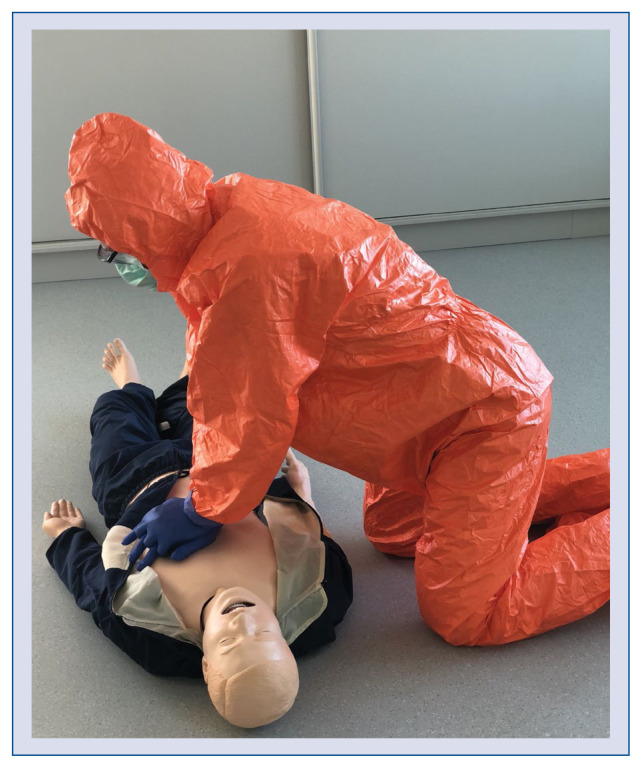
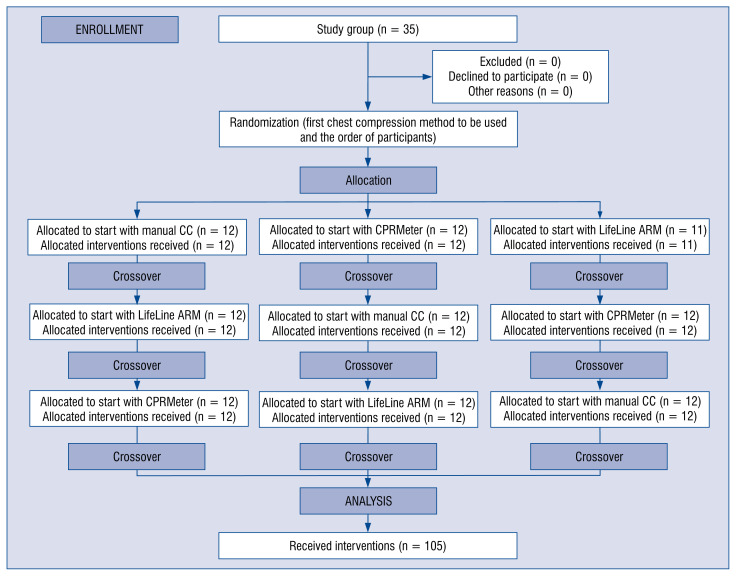
Methods: This was prospective, randomized, multicenter, single-blinded, crossover simulation trial. Thirty-five medical students after an advanced cardiovascular life support course, which included performing 2-min continuous chest compression scenarios using three methods: (A) manual chest compression (CC), (B) compression with CPRMeter, (C) compression with LifeLine ARM device. During resuscitation they are wearing full personal protective equipment for aerosol generating procedures.
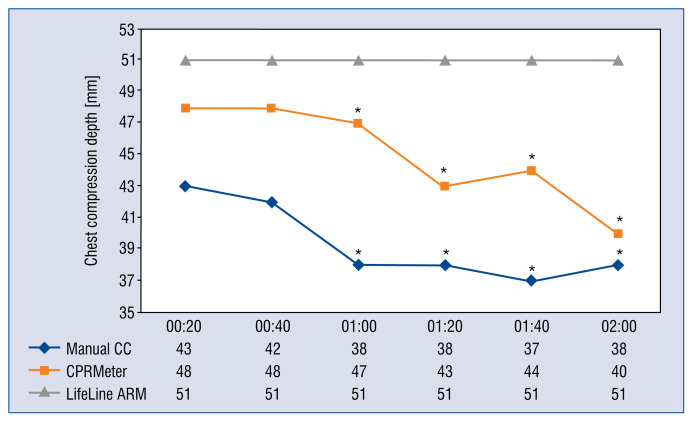
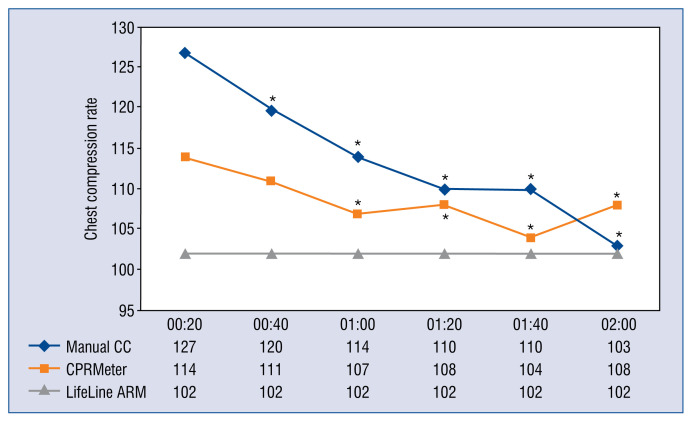
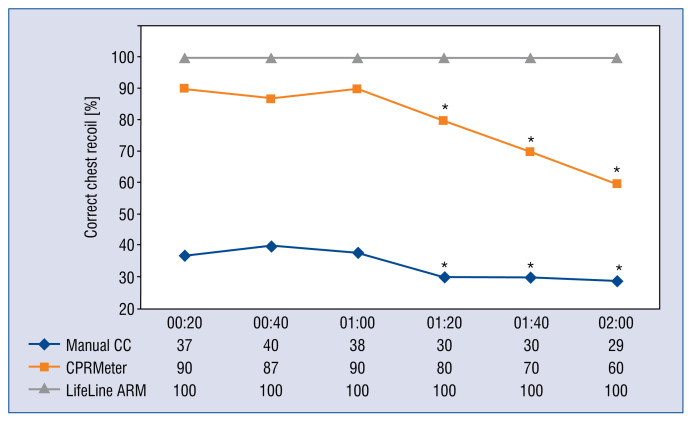
Results: The median chest compression depth using manual CC, CPRMeter and LifeLine ARM varied and amounted to 40 (38-45) vs. 45 (40-50) vs. 51 (50-52) mm, respectively (p = 0.002). The median chest compression rate was 109 (IQR; 102-131) compressions per minute (CPM) for manual CC, 107 (105-127) CPM for CPRMeter, and 102 (101-102) CPM for LifeLine ARM (p = 0.027). The percentage of correct chest recoil was the highest for LifeLine ARM - 100% (95-100), 80% (60-90) in CPRMeter group, and the lowest for manual CC - 29% (26-48).
Conclusions: According to the results of this simulation trial, automated chest compression devices (ACCD) should be used for chest compression of patients with suspected/confirmed COVID-19. In the absence of ACCD, it seems reasonable to change the cardiopulmonary resuscitation algorithm (in the context of patients with suspected/confirmed COVID-19) by reducing the duration of the cardiopulmonary resuscitation cycle from the current 2-min to 1-min cycles due to a statistically significant reduction in the quality of chest compressions among rescuers wearing PPE AGP.
Keywords: COVID-19; SARS-CoV-2; cardiopulmonary resuscitation; chest compression; medical simulation; quality.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
