

Detection and management of arrhythmias in peripartum cardiomyopathy
- PMID: 32420115
- PMCID: PMC7225429
- DOI: 10.21037/cdt.2019.05.03
Detection and management of arrhythmias in peripartum cardiomyopathy
Abstract
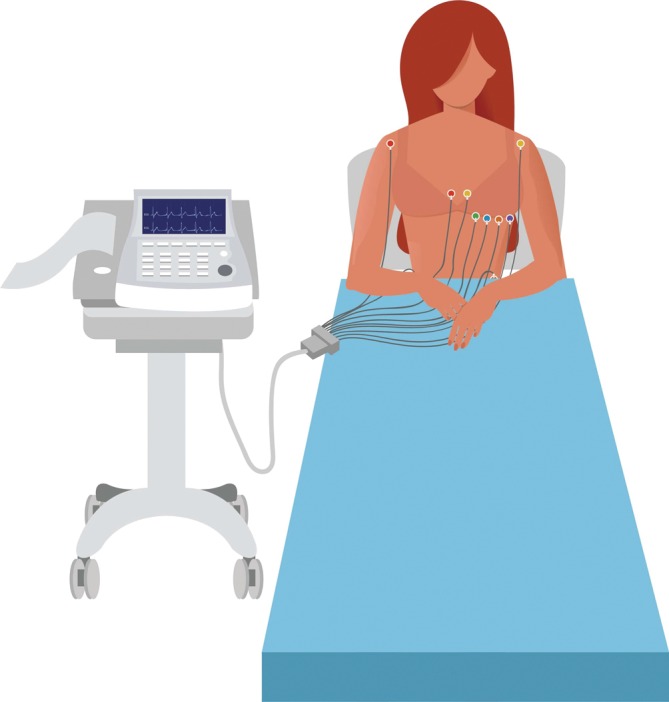
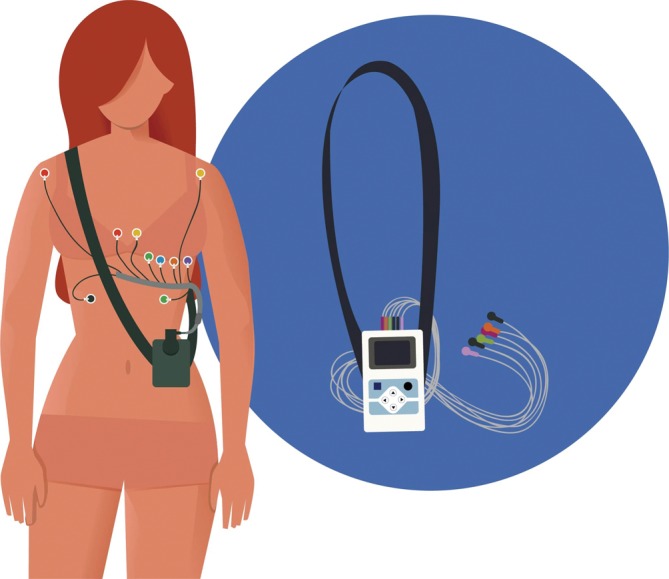
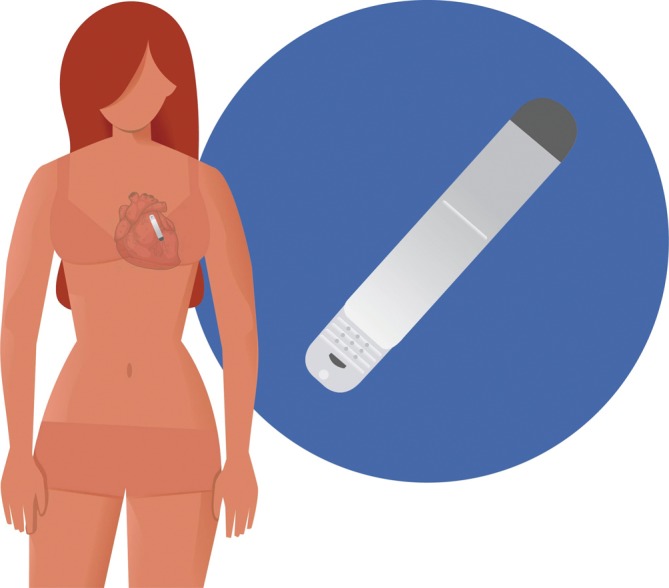
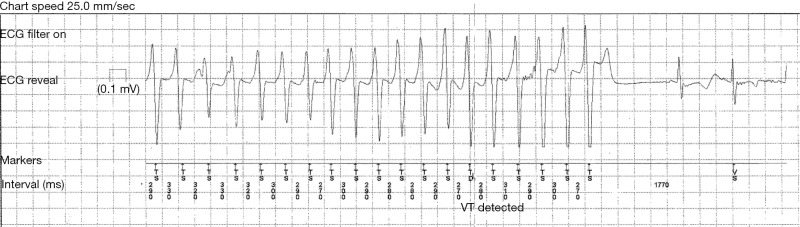
Peripartum cardiomyopathy (PPCM) is an idiopathic dilated cardiomyopathy, in which previously healthy women present with heart failure secondary to left ventricular (LV) systolic dysfunction during the last months of pregnancy or up to 5 months postpartum. PPCM occurs worldwide. The incidence seems to be increasing, possibly due to increasing awareness of the condition and diagnosis thereof. Women diagnosed with PPCM present with symptoms and signs of heart failure, thromboembolism or arrhythmia. Although the incidence of arrhythmias in this condition is not well documented, patients with PPCM often have rhythm disturbances. Indeed, life-threating arrhythmias contribute significantly to sudden cardiac death (SCD) in this population, especially when patients have poor systolic function. In this review, we summarize the evidence on atrial and ventricular arrhythmias in PPCM, as detected by various diagnostic modalities. Furthermore, we summarize the management of arrhythmias in PPCM, as recommended by contemporary guidelines.
Keywords: Ambulatory electrocardiographic monitoring (AECG); arrhythmia; cardioverter-defibrillator; electrocardiogram (ECG); peripartum cardiomyopathy (PPCM).
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt.2019.05.03). The series “Cardiovascular Diseases in Low-and Middle-Income Countries” was commissioned by the editorial office without any funding or sponsorship. The authors have no conflicts of interest to declare.
Figures
References
-
- Sliwa K, Hilfiker-Kleiner D, Petrie MC, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Eur J Heart Fail 2010;12:767-78. 10.1093/eurjhf/hfq120 - DOI - PubMed
-
- Isezuo SA, Abubakar SA. Epidemiologic profile of peripartum cardiomyopathy in a tertiary care hospital. Ethn Dis 2007;17:228-33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources