

A glimpse of hope: cardiac surgery in low- and middle-income countries (LMICs)
- PMID: 32420116
- PMCID: PMC7225428
- DOI: 10.21037/cdt.2019.11.03
A glimpse of hope: cardiac surgery in low- and middle-income countries (LMICs)
Abstract
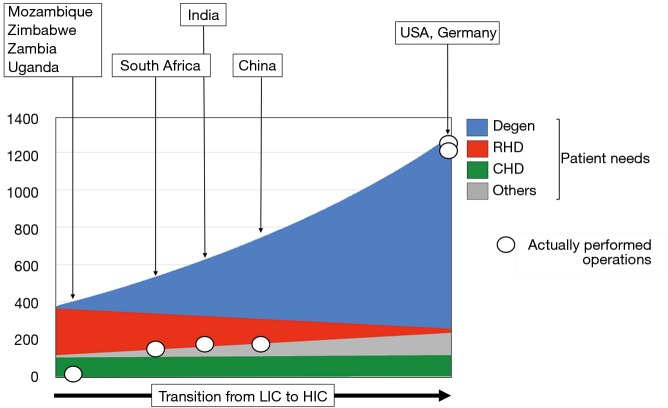
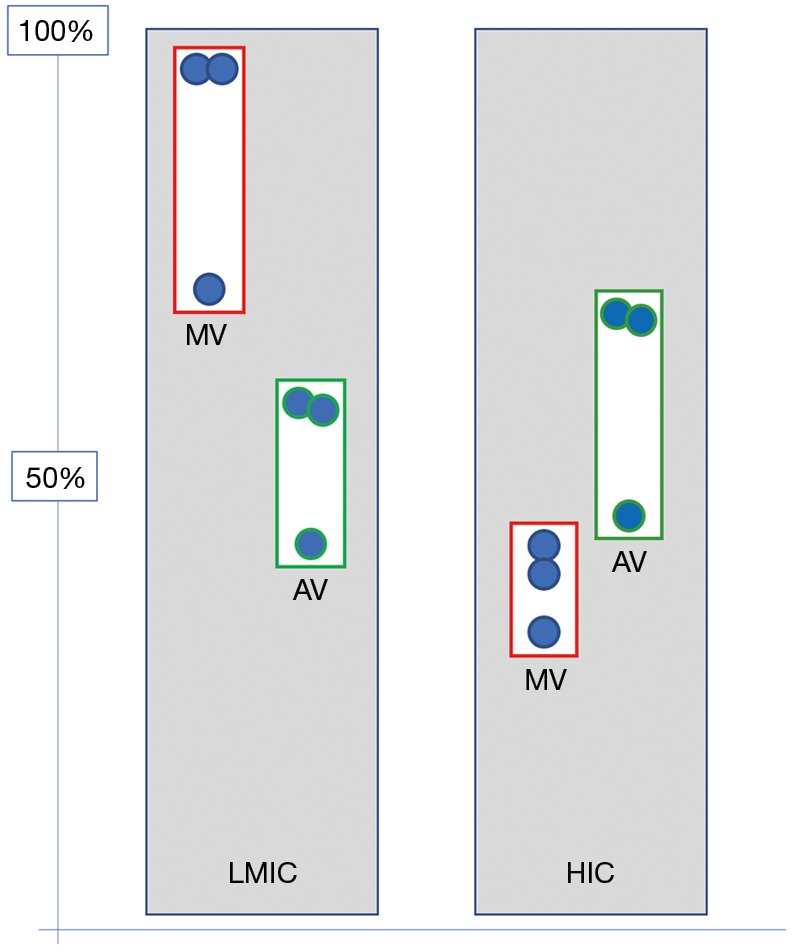
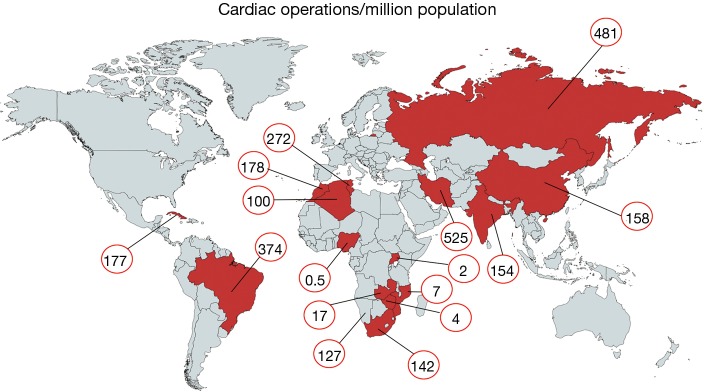
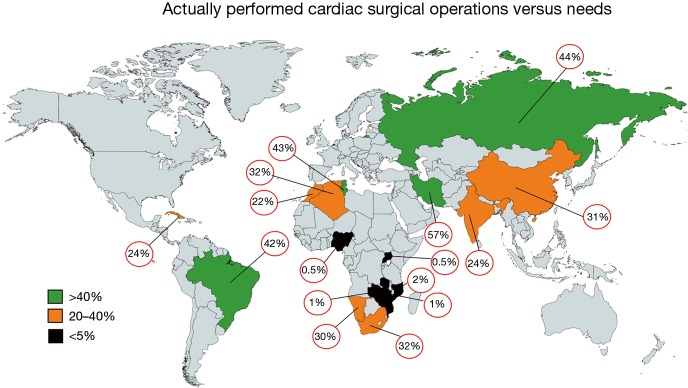
Currently, more than five times more people live in low- and middle-income countries (LMICs) than in high-income countries (HICs). As such, the downward trend in cardiac surgical needs in HICs reflects only the situation of one sixth of the world population while the vast majority living in LMICs has still no or limited access to life saving heart operations. In these countries, rheumatic heart disease (RHD) still accounts for a significant proportion of cardiac surgical needs. In low- and lower-middle income countries it remains the single most common cardiovascular disease in young adult and adolescent patients in need of heart surgery outweighing other indications such as congenital cardiac defects almost 4-fold. Compared to HICs with their predominance of calcific aortic stenosis in the elderly mitral valve surgery is required in >90% of the largely young patients with RHD in low-income countries (LICs) and still in 70% of the often middle aged patients in middle-income countries (MICs). Although recent government initiatives in LICs led to the establishment of local, independent cardiac surgical services gradually replacing fly-in missions, these centers still only cover less than 2% of the needs of their populations. In MICs, cardiac surgical needs continually grow with the emergence of degenerative diseases. As such, in spite of the concomitant growth of cardiac surgical capacity, significantly less than half the estimated patients in need have access. Capacities in LICs range from 0.5 to 7 cardiac operations/million population; 100-481/million in MICs and >1,200/million in HICs such as the USA and Germany. While a new level of awareness of the scope and magnitude of the problem has begun to emerge in LICs and the establishment of local cardiac surgical capacity has given rise to a glimpse of hope, the challenges of expanding these fledgling services to a significant proportion of the population still seem insurmountable. Challenges in MICs are on the other hand the widening gap between private cardiac medicine for the affluent few and overwhelmed public services for the many and the rural urban divide with the underappreciation of the ongoing dominance of RHD in the rural and indigent population on the other. Overshadowing all LMICs is the low level of valve-repair skills associated with insufficient cardiac surgical capacity and the unavailability of suitable replacement valves which address the young age of the patients and the difficulties of anticoagulation in a socioeconomic environment distinctly different from the elderly patients of HICs.
Keywords: Cardiac surgical needs; low- and middle-income countries (LMICs); operative capacity.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt.2019.11.03). The series “Cardiovascular Diseases in Low-and Middle-Income Countries” was commissioned by the editorial office without any funding or sponsorship. The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous