

Case report: IgG4-related renal disease co-existing with retroperitoneal fibrosis
- PMID: 32420186
- PMCID: PMC7215037
- DOI: 10.21037/tau.2020.02.06
Case report: IgG4-related renal disease co-existing with retroperitoneal fibrosis
Abstract
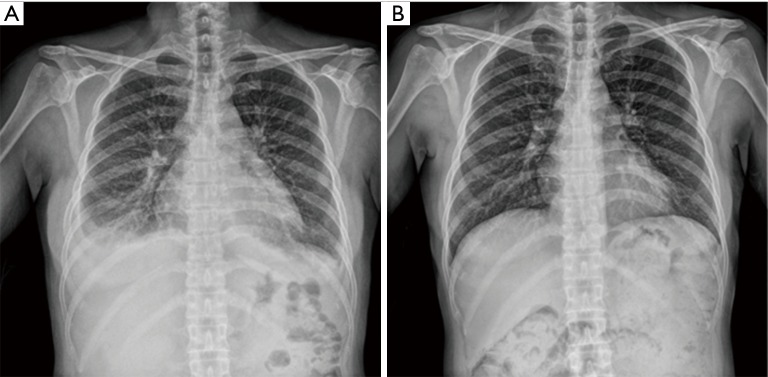
A 51-year-old woman visited our clinic for orthopnea, chest discomfort, and facial and leg edema. Acute kidney injury and pleural effusion were diagnosed and she received hemodialysis. This is a rare case of IgG4-related disease diagnosed by renal biopsy in the patient with retroperitoneal fibrosis and severe acute kidney injury, which progressed rapidly and required hemodialysis without markedly elevated serum IgG4 level and urinary tract obstruction. Immunostaining of a kidney biopsy revealed IgG4-related renal disease and magnetic resonance imaging showed retroperitoneal fibrosis in the paraspinal and presacral areas. After 3 days of glucocorticoid treatment, renal function and bilateral pleural effusion were restored. Another 2 months of glucocorticoid treatment decreased the extent of retroperitoneal fibrosis on follow-up abdominal computed tomography. IgG4-related disease is a recently recognized fibro-inflammatory condition with a dense lymphoplasmacytic infiltration of IgG4-positive plasma cells. The kidney and retroperitoneum are the frequently associated organs in IgG4-related disease. This case shows that IgG4-related disease can involve the kidney and/or other organs and be diagnosed by kidney biopsy.
Keywords: IgG4-related renal disease; acute kidney injury; case report; kidney biopsy; retroperitoneal fibrosis.
2020 Translational Andrology and Urology. All rights reserved.
Conflict of interest statement
Conflict of interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tau.2020.02.06). The authors have no conflicts of interest to declare.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources