

Posterior reversible encephalopathy syndrome in an oncological normotensive patient: evidence for a pathogenic role of concomitant low magnesium serum levels and chemotherapy treatment
- PMID: 32420975
- PMCID: PMC7569613
- DOI: 10.23750/abm.v91i2.8685
Posterior reversible encephalopathy syndrome in an oncological normotensive patient: evidence for a pathogenic role of concomitant low magnesium serum levels and chemotherapy treatment
Abstract
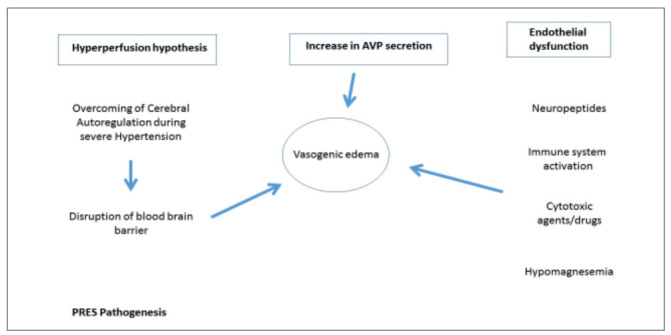
Background: Posterior reversible encephalopathy (PRES) is a rare syndrome characterized by headache, confusion, seizures, visual changes and white matter edema at radiological imaging. Its pathophysiology is not clarified and different causes, including uncontrolled hypertension, eclampsia, chemotherapy and hypomagnesemia have been suggested.
Case report: A woman affected by stage IV breast cancer with lower extremity deep vein thrombosis treated with low-molecular-weight-heparin, currently in therapy with Palbociclib/Fulvestrant (antiCDK4 and 6/estrogen receptor antagonist) but previously treated with several other chemotherapy lines (including VEGF inhibitor bevacizumab), was admitted to our Internal Medicine department because of ascites and abdominal pain. She was treated with diuretics (and paracentesis). Recently (six-month earlier) a pan-encephalic radiotherapy was done because of brain and skull metastasis. Among blood tests, low serum levels of hypomagnesemia were observed. She developed PRES that rapidly progressed to lethargy, unresponsiveness till coma without changes in blood pressure. Magnetic Resonance Imaging study showed bilateral parieto-occipital edema and a thrombosis of left transverse and sigmoid sinuses. Anti-edema therapy, intravenous supplementation of magnesium and decoagulation were started, with complete and rapid recovery (within 18 hours) of clinical and radiologic changes.
Conclusions: PRES diagnosis was based on the rapid clinical recovery after antiedema treatment and magnesium supplementation. Low magnesium level related to both diuretic and Fulvestrant/Palbociclib therapies and recent radiotherapy can represent potential mechanisms favouring PRES development. The previous bevacizumab treatment may also be involved as a PRES predisposing factor. The concomitant occurrence of cerebral thrombosis can have precipitated the clinical situation.
Conflict of interest statement
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
Figures




Similar articles
-
Posterior reversible encephalopathy syndrome due to malignant hypercalcemia: physiopathological considerations.J Clin Endocrinol Metab. 2014 Apr;99(4):1112-6. doi: 10.1210/jc.2013-3487. Epub 2014 Jan 29. J Clin Endocrinol Metab. 2014. PMID: 24476076
-
Chemotherapy-induced posterior reversible encephalopathy syndrome: Three case reports.Medicine (Baltimore). 2019 May;98(19):e15691. doi: 10.1097/MD.0000000000015691. Medicine (Baltimore). 2019. PMID: 31083272 Free PMC article.
-
Variant Type of Posterior Reversible Encephalopathy Syndrome Associated with Deep Brain Hemorrhage: Case Report and Review of the Literature.World Neurosurg. 2020 Feb;134:176-181. doi: 10.1016/j.wneu.2019.10.196. Epub 2019 Nov 8. World Neurosurg. 2020. PMID: 31712110 Review.
-
Posterior Reversible Encephalopathy Syndrome in Patients With Cancer.Oncologist. 2015 Jul;20(7):806-11. doi: 10.1634/theoncologist.2014-0149. Epub 2015 Jun 1. Oncologist. 2015. PMID: 26032137 Free PMC article.
-
Posterior reversible encephalopathy syndrome possibly induced by pemetrexed maintenance therapy for lung cancer: a case report and literature review.Acta Clin Belg. 2018 Oct;73(5):382-388. doi: 10.1080/17843286.2017.1403103. Epub 2017 Nov 24. Acta Clin Belg. 2018. PMID: 29173113 Review.
Cited by
-
Posterior Reversible Encephalopathy Occurring During Treatment With Palbociclib.Cureus. 2021 Jul 24;13(7):e16604. doi: 10.7759/cureus.16604. eCollection 2021 Jul. Cureus. 2021. PMID: 34447643 Free PMC article.
-
A Rare Association of Hypomagnesemia and Posterior Reversible Encephalopathy Syndrome (PRES).Cureus. 2023 Jul 8;15(7):e41572. doi: 10.7759/cureus.41572. eCollection 2023 Jul. Cureus. 2023. PMID: 37554607 Free PMC article.
-
Management and Clinical Outcome of Posterior Reversible Encephalopathy Syndrome in Pediatric Oncologic/Hematologic Diseases: A PRES Subgroup Analysis With a Large Sample Size.Front Pediatr. 2021 Jul 1;9:678890. doi: 10.3389/fped.2021.678890. eCollection 2021. Front Pediatr. 2021. PMID: 34277519 Free PMC article.
-
Posterior Reversible Encephalopathy Syndrome Induced by Hypomagnesemia due to Clostridium Difficile in a Patient with Kidney Transplant.Case Rep Neurol. 2021 Oct 22;13(3):693-698. doi: 10.1159/000519883. eCollection 2021 Sep-Dec. Case Rep Neurol. 2021. PMID: 34899254 Free PMC article.
-
Posterior reversible encephalopathy syndrome associated with use of anlotinib to treat squamous cell carcinoma of the cervix: case report and literature review.Front Pharmacol. 2023 Dec 15;14:1255785. doi: 10.3389/fphar.2023.1255785. eCollection 2023. Front Pharmacol. 2023. PMID: 38169843 Free PMC article.
References
-
- Hinchey J, Chaves C, Appignani B, et al. A Reversible Posterior Leukoencephalopathy syndrome. N Engl J Med. 1996:494–500. - PubMed
-
- Stott V, Hurrell M, Anderson TJ. Reversible posterior leukoencephalopathy syndrome: a misnomer reviewed. Intern Med J. 2005;35(2):83–90. - PubMed
-
- Siebert E, Bohner G, Liebig T, Endres M, Liman TG. Factors associated with fatal outcome in posterior reversible encephalopathy syndrome: a retrospective analysis of the Berlin PRES study. J Neurol. 2017;264(2):237–242. - PubMed
-
- Ay H, Buonanno F, Schaefer P, et al. Posterior leukoencephalopathy without severe hypertension: utility of diffusion-weighted MRI. Neurology. 1998;51(5):1369–1376. - PubMed
-
- Mar GR. Encefalopatía reversible posterior en una niña con lupus eritematoso sistémico. Presentación de un caso. Arch Argent Pediatr. 2015;113(5):271–274. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
