

Characterization of on-target adverse events caused by TRK inhibitor therapy
- PMID: 32422171
- PMCID: PMC8341080
- DOI: 10.1016/j.annonc.2020.05.006
Characterization of on-target adverse events caused by TRK inhibitor therapy
Abstract
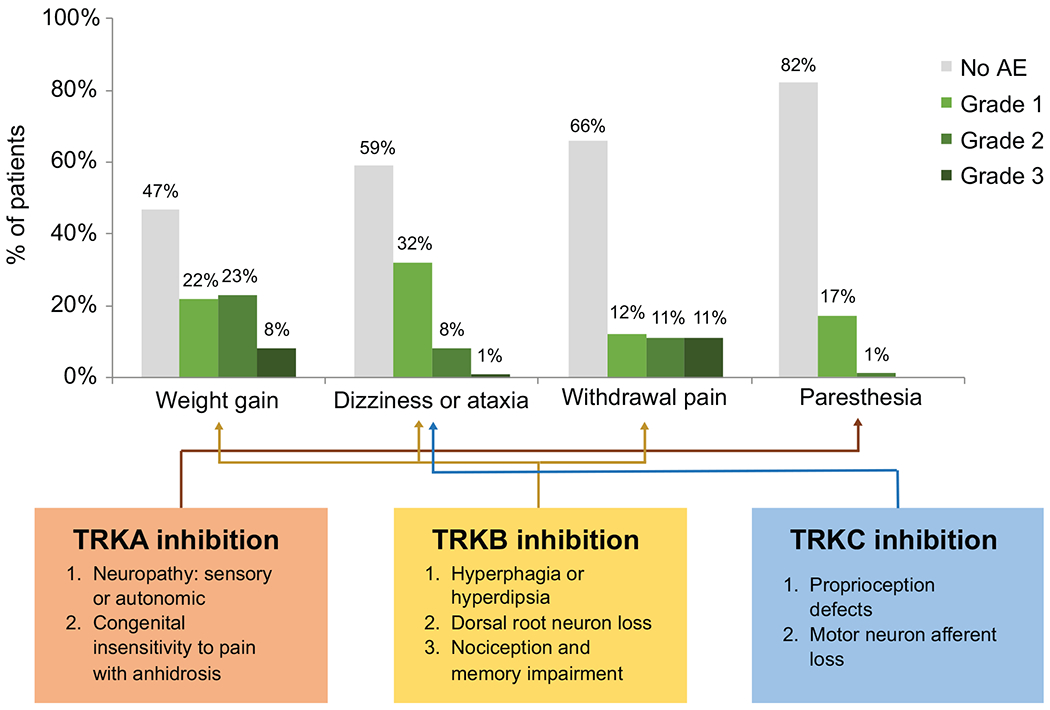
Background: The tropomyosin receptor kinase (TRK) pathway controls appetite, balance, and pain sensitivity. While these functions are reflected in the on-target adverse events (AEs) observed with TRK inhibition, these AEs remain under-recognized, and pain upon drug withdrawal has not previously been reported. As TRK inhibitors are approved by multiple regulatory agencies for TRK or ROS1 fusion-positive cancers, characterizing these AEs and corresponding management strategies is crucial.
Patients and methods: Patients with advanced or unresectable solid tumors treated with a TRK inhibitor were retrospectively identified in a search of clinical databases. Among these patients, the frequency, severity, duration, and management outcomes of AEs including weight gain, dizziness or ataxia, and withdrawal pain were characterized.
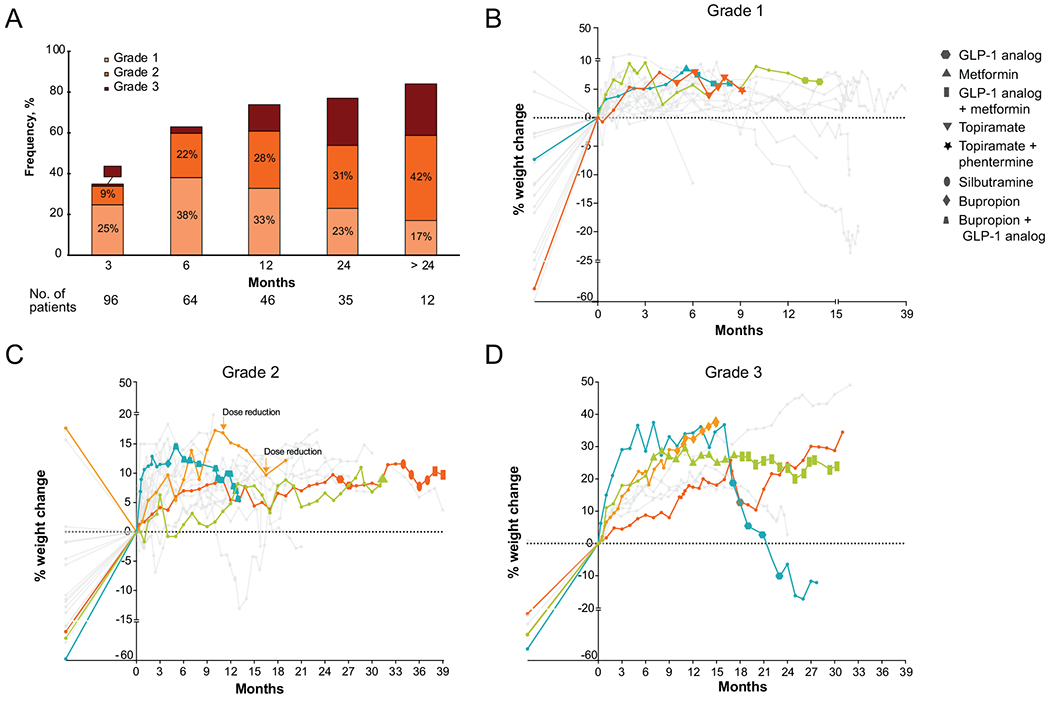
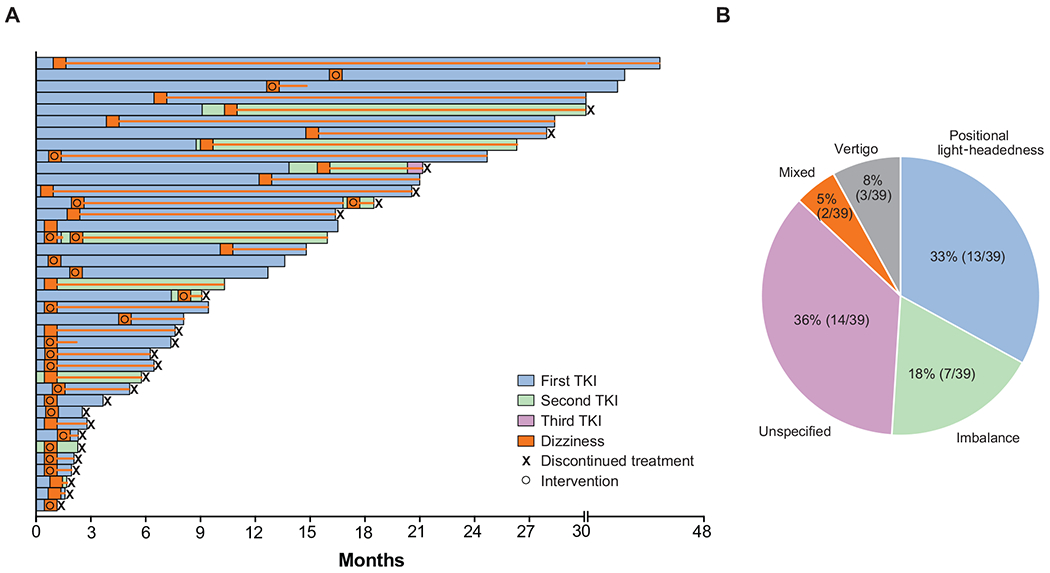
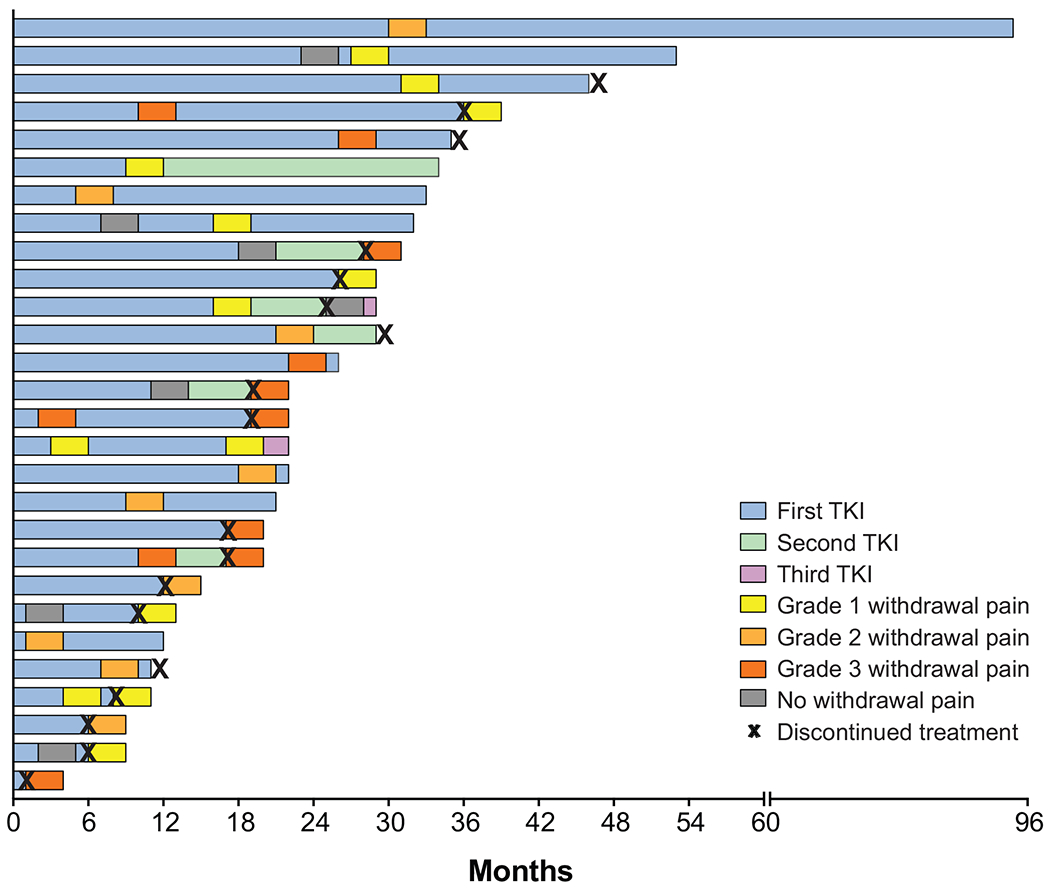
Results: Ninety-six patients with 15 unique cancer histologies treated with a TRK inhibitor were identified. Weight gain was observed in 53% [95% confidence interval (CI), 43%-62%] of patients and increased with time on TRK inhibition. Pharmacologic intervention, most commonly with glucagon-like peptide 1 analogs or metformin, appeared to result in stabilization or loss of weight. Dizziness, with or without ataxia, was observed in 41% (95% CI, 31%-51%) of patients with a median time to onset of 2 weeks (range, 3 days to 16 months). TRK inhibitor dose reduction was the most effective intervention for dizziness. Pain upon temporary or permanent TRK inhibitor discontinuation was observed in 35% (95% CI, 24%-46%) of patients; this was more common with longer TRK inhibitor use. TRK inhibitor reinitiation was the most effective intervention for withdrawal pain.
Conclusions: TRK inhibition-related AEs including weight gain, dizziness, and withdrawal pain occur in a substantial proportion of patients receiving TRK inhibitors. This safety profile is unique relative to other anticancer therapies and warrants careful monitoring. These on-target toxicities are manageable with pharmacologic intervention and dose modification.
Keywords: NTRK fusion; TRK inhibitors; toxicity management.
Copyright © 2020 European Society for Medical Oncology. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Disclosure JF has received honoraria from Genentech. AL has received research funding from Bristol Myers Squibb and NantOmics and holds equity in Sanofi. MO has served on advisory boards for PharmaMar, Novartis, and Targeted Oncology, and received travel expenses from Bristol Myers Squibb and Merck. YRM-G has received travel expenses from AstraZeneca. BTL holds two institutional patents (US62/685,057, US62/514,661), and has served on advisory boards for Genentech (subsidiary of Roche), Eli Lilly, Guardant Health, Hengrui Therapeutics, Mersana Therapeutics, and Thermo Fisher Scientific, received travel expenses from MORE Health and Resolution Bioscience, and received research funding from Amgen, AstraZeneca, BioMedValley Discoveries, Daiichi Sankyo, Genentech, GRAIL, Guardant Health, Eli Lilly, Hengrui Therapeutics, Illumina, and MORE Health. JJH has received consulting fees from Bristol Myers Squibb, Cytomx, Eli Lilly, Eisai, Exelixis, Imvax, QED, and research funding from Bristol Myers Squibb. GI has received research funding from Janssen, Mirati Therapeutics, and Novartis, and consulting fees from Mirati Therapeutics. MMG has received honoraria from Bayer and Flatiron Health, served on advisory boards for Bayer, Boehringer Ingelheim, Epizyme, Daiichi Sankyo, Karyopharm, and Springworks Therapeutics, served on a speakers’ bureau for Amgen, and received travel expenses from Epizyme. AS has received research funding from Eli Lilly, Kura Oncology, Merus, Northern Biologics, and Surface Oncology. DMH owns stock in Fount Therapeutics, has served on advisory boards for ArQule, AstraZeneca, Bayer, Boehringer Ingelheim, Chugai Pharma, CytomX, Debiopharm, Fount Therapeutics, Genentech, Eli Lilly, Janssen, Jazz Pharma, Pfizer, and Puma Biotechnology, received research funding from AstraZeneca, Bayer, Loxo Oncology, and Puma Biotechnology, and received travel expenses from Chugai Pharma and Genentech; he is currently employed by and holds equity in Loxo Oncology, a subsidiary of Eli Lilly. AD has received honoraria and/or served on advisory boards for 14ner/Elevation Oncology, Abbvie, ArcherDX, AstraZeneca, Axis Pharma, Bayer, Beigene, BergenBio, Blueprint Medicines, Exelixis, Helsinn, Hengrui Therapeutics, Loxo Oncology (subsidiary of Eli Lilly), Monopteros, MORE Health, Remedica, Roche (subsidiaries Genentech and Ignyta), Pfizer, Takeda (subsidiaries Ariad and Millennium), TP Therapeutics, Tyra Biosciences, and Verastem; and received research funding from Exelixis, Foundation Medicine GlaxoSmithKline, Pfizer, PharmaMar, Teva, and Taiho. All research funding was provided to the institution. All other authors report no financial relationships.
Figures
Comment in
-
TRK inhibitors: managing on-target toxicities.Ann Oncol. 2020 Sep;31(9):1109-1111. doi: 10.1016/j.annonc.2020.06.010. Epub 2020 Jun 20. Ann Oncol. 2020. PMID: 32574723 No abstract available.
References
-
- Demetri GD, Paz-Ares L, Farago AF et al. Efficacy and safety of entrectinib in patients with NTRK fusion-positive tumours: Pooled analysis of STARTRK-2, STARTRK-1, and ALKA-372-001. Annals of Oncology 2018; 29.
-
- Hyman D, Kummar S, Farago A et al. Phase I and expanded access experience of LOXO-195 (BAY 2731954), a selective next-generation TRK inhibitor (TRKi). Cancer Res 2019; 79: CT127.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
