

Tension pneumothorax in a patient with COVID-19
- PMID: 32423911
- PMCID: PMC7239515
- DOI: 10.1136/bcr-2020-235861
Tension pneumothorax in a patient with COVID-19
Abstract
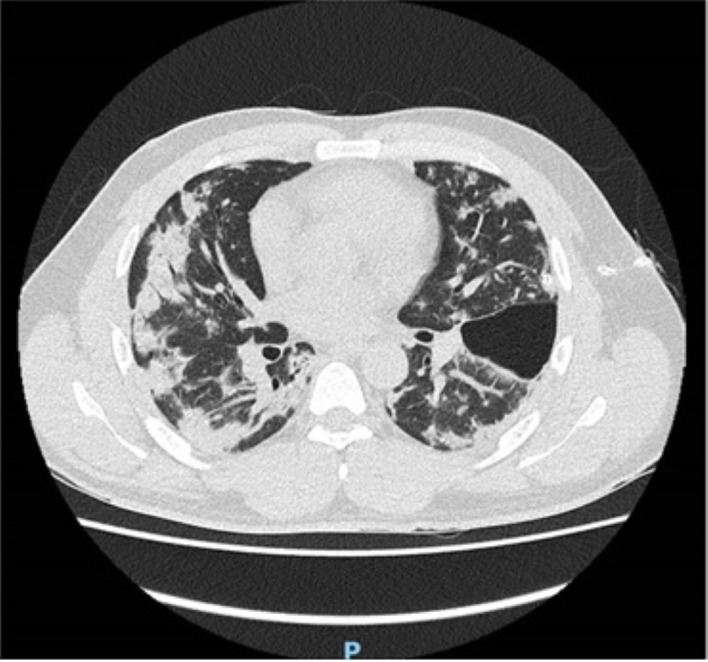
A 36-year-old man was brought to the emergency department with suspected COVID-19, following a 3-week history of cough, fevers and shortness of breath, worsening suddenly in the preceding 4 hours. On presentation he was hypoxaemic, with an SpO2 of 88% on 15 L/min oxygen, tachycardic and had no audible breath sounds on auscultation of the left hemithorax. Local guidelines recommended that the patient should be initiated on continuous positive airway pressure while investigations were awaited, however given the examination findings an emergency portable chest radiograph was performed. The chest radiograph demonstrated a left-sided tension pneumothorax. This was treated with emergency needle decompression, with good effect, followed by chest drain insertion. A repeat chest radiograph demonstrated lung re-expansion, and the patient was admitted to a COVID-19 specific ward for further observation. This case demonstrates tension pneumothorax as a possible complication of suspected COVID-19 and emphasises the importance of thorough history-taking and clinical examination.
Keywords: emergency medicine; infectious diseases; intensive care; respiratory medicine.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Huang Y, Wang S, Liu Y, et al. . A preliminary study on the ultrasonic manifestations of Peripulmonary lesions of Non-Critical novel coronavirus pneumonia (COVID-19). SSRN Electronic Journal 2020. 10.2139/ssrn.3544750 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical