

Association of dairy consumption with metabolic syndrome, hypertension and diabetes in 147 812 individuals from 21 countries
- PMID: 32423962
- PMCID: PMC7326257
- DOI: 10.1136/bmjdrc-2019-000826
Association of dairy consumption with metabolic syndrome, hypertension and diabetes in 147 812 individuals from 21 countries
Abstract
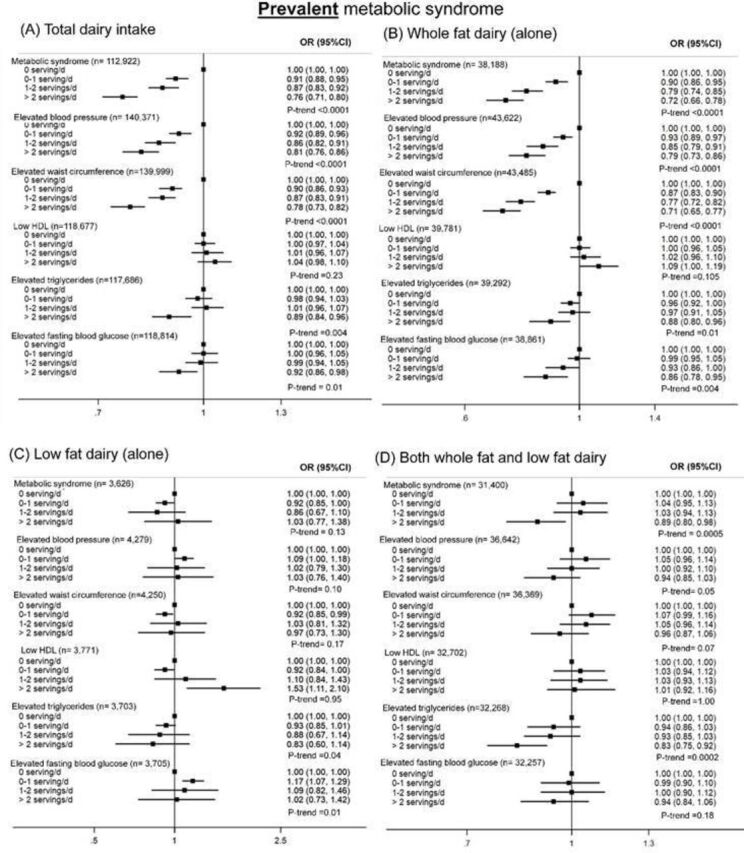
Objective: Our aims were to assess the association of dairy intake with prevalence of metabolic syndrome (MetS) (cross-sectionally) and with incident hypertension and incident diabetes (prospectively) in a large multinational cohort study.
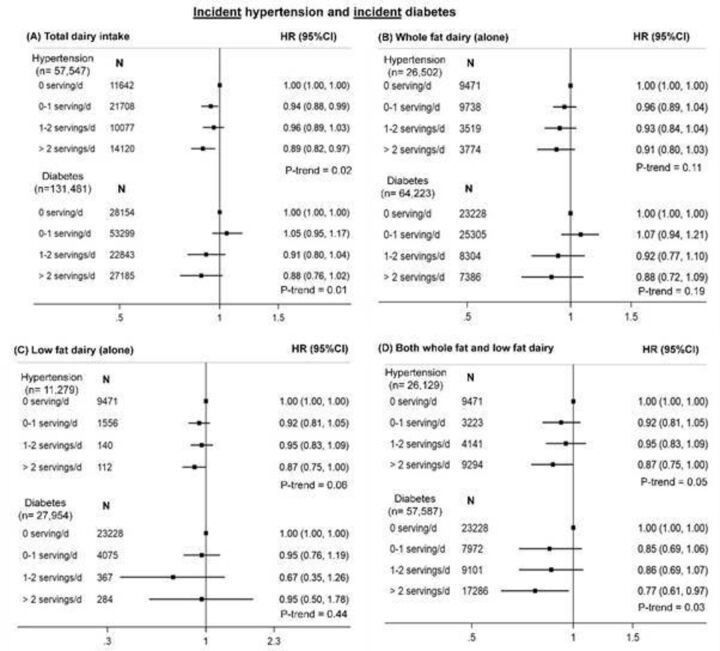
Methods: The Prospective Urban Rural Epidemiology (PURE) study is a prospective epidemiological study of individuals aged 35 and 70 years from 21 countries on five continents, with a median follow-up of 9.1 years. In the cross-sectional analyses, we assessed the association of dairy intake with prevalent MetS and its components among individuals with information on the five MetS components (n=112 922). For the prospective analyses, we examined the association of dairy with incident hypertension (in 57 547 individuals free of hypertension) and diabetes (in 131 481 individuals free of diabetes).
Results: In cross-sectional analysis, higher intake of total dairy (at least two servings/day compared with zero intake; OR 0.76, 95% CI 0.71 to 0.80, p-trend<0.0001) was associated with a lower prevalence of MetS after multivariable adjustment. Higher intakes of whole fat dairy consumed alone (OR 0.72, 95% CI 0.66 to 0.78, p-trend<0.0001), or consumed jointly with low fat dairy (OR 0.89, 95% CI 0.80 to 0.98, p-trend=0.0005), were associated with a lower MetS prevalence. Low fat dairy consumed alone was not associated with MetS (OR 1.03, 95% CI 0.77 to 1.38, p-trend=0.13). In prospective analysis, 13 640 people with incident hypertension and 5351 people with incident diabetes were recorded. Higher intake of total dairy (at least two servings/day vs zero serving/day) was associated with a lower incidence of hypertension (HR 0.89, 95% CI 0.82 to 0.97, p-trend=0.02) and diabetes (HR 0.88, 95% CI 0.76 to 1.02, p-trend=0.01). Directionally similar associations were found for whole fat dairy versus each outcome.
Conclusions: Higher intake of whole fat (but not low fat) dairy was associated with a lower prevalence of MetS and most of its component factors, and with a lower incidence of hypertension and diabetes. Our findings should be evaluated in large randomized trials of the effects of whole fat dairy on the risks of MetS, hypertension, and diabetes.
Keywords: adult diabetes; endocrinology; hypertension; nutrition.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International diabetes Federation Task force on epidemiology and prevention; National heart, lung, and blood Institute; American heart association; world heart Federation; international atherosclerosis Society; and international association for the study of obesity. Circulation 2009;120:1640–5. 10.1161/CIRCULATIONAHA.109.192644 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical