

Improving the use of the 'COUGH' bundle in Surgical High Dependency Unit, Ninewells Hospital, Dundee
- PMID: 32423972
- PMCID: PMC7245369
- DOI: 10.1136/bmjoq-2019-000851
Improving the use of the 'COUGH' bundle in Surgical High Dependency Unit, Ninewells Hospital, Dundee
Abstract
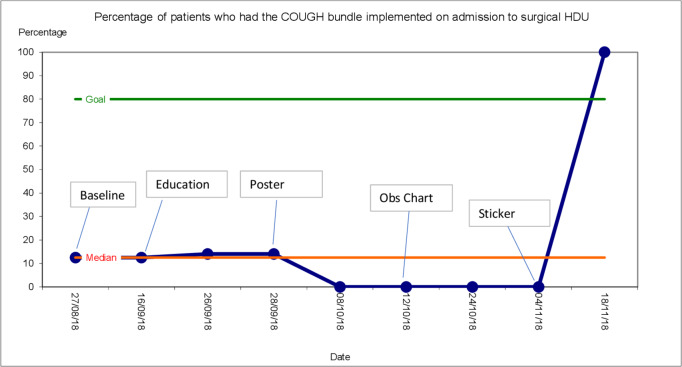
Developing respiratory complications postoperatively is one of the major determinants of longer hospital stay, morbidity, mortality and increased healthcare costs. The incidence of postoperative respiratory complications varies from 1% to 23%. Given that postoperative respiratory complications are relatively common and costly, there have been various studies which look at ways to reduce the risk of these occurring. One such protocol is the ICOUGH bundle which stands for Incentive spirometry, Coughing and deep breathing, Oral care, patient Understanding, Getting out of bed and Head of bed elevation. This has been adapted locally to the Coughing and deep breathing, Oral care, patient Understanding, Getting out of bed and Head of bed elevation (COUGH) bundle which consists of these components excluding incentive spirometry. Within our surgical high dependency unit (HDU), the COUGH bundle should be implemented in patients who have a moderate or high risk of developing postoperative respiratory complications with an Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score of 26 or above. Studies have shown that the ICOUGH bundle has reduced rates of pneumonia and unplanned intubation in general surgical and vascular patients. Baseline data taken from surgical HDU showed that the COUGH bundle was not well implemented. One out of eight patients who had an ARISCAT score greater than 26 had the COUGH bundle implemented on admission to the unit. Three out of eight patients had the ARISCAT score documented in their admission medical review. One patient who should have received the bundle, but did not, developed a hospital acquired pneumonia postoperatively. To address this issue, we aimed to increase awareness surrounding the COUGH bundle and to increase the number of patients who had the COUGH bundle started on admission. This quality improvement project had four cycles (plan, do, study, act) and after these, 100% of patients who had an ARISCAT score of 26 or more had the COUGH bundle implemented.
Keywords: PDSA; critical care; healthcare quality improvement; patient-centred care; quality improvement.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical